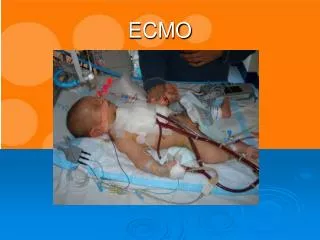
ECMO
ECMO, cardiac shock, respiratory failure

ECMO
E N D
Presentation Transcript
Extracorporeal Membrane Oxygenation Dr. Pham Dang Hai
Definition • External artificial circuit carries venous blood from the patient to an oxygenator. • Blood becomes enriched with oxygen and has carbon dioxide removed. • The blood is than returned to the patient via a central vein or an artery.
Introduction Extra corporeal Life Support is achieved by : - Draining venous blood - Removing CO2 - Adding oxygen - Returning to circulation - Through either a vein or artery
The physiologic goal is to improve tissue oxygen delivery , remove CO2 and allow normal aerobic metabolism whilst the lung rests • ECMO circulation: - Dual circulation - Nonpulsatile flow
Evolution of ECMO • BARTLETT –Father of ECMO • 1975-: Successfully applied bed side ECLS device to treat newborn with meconium aspiration. • Developed of better membrane oxygenators.
First successful ECMO patient, 1971 J Donald Hill MD and Maury Bramson BME, Santa Barbara, Ca, 1971. (Courtesy of Robert Bartlett, MD)
First Neonatal ECMO survivor.. “The Hope” ESPERANZA-1975
FROM THIS TO THIS
Evolution of ECMO • 1989-: Over 100 ECMO centers across the world established Extracorporeal Life Support Organization (ELSO). • Platform of communication and research.
Modes of ECMO ECMO can be categorized according to the circuit used • Veno-arterial - VA ECMO provides both gas exchange and circulatory support (Heart & Lung failure) • Veno-venous –VV ECMO allows gas exchange only (Isolated Lung failure)
Indications of ECMO for cardiogenic shock • Epinephrine > 0.2 μg/kg/min or dobutamine > 20 μg/kg/min ± norepinephrine > 0.2 μg/kg/min) • preload optimization • Low cardiac output: (cardiac index <2.2 L/min/m2 + LVEF <20 % + AVTI < 8 cm • Persistent tissue hypoxia
33% 60%
Inclusion criteria • Presence of any two of the criteria from the following observed over a period of 4 to 6 hours after maximum medical resuscitation. • PaO2/FiO2 <75% • Oxygen index >40% • Murrays Score of >3 • aA gradient >600 • Hypercapnia with PH of <7.2 observed over more than 3 hours. • Lung compliance <0.5 cc/cmH2O/kg
Absolute Contraindications to all forms of ECMO • Age: > 70 years • Active malignancy • Severe brain injury • Previous Bone marrow transplant, previous transplant (>30 days). • AIDS • End stage chronic organ failure (hepatic, renal)
Absolute Contraindications to all forms of ECMO • End stage cardiomyopathy (except for bridge to VAD/transplant) • Chronic lung disease (except for bridge to transplant) • Multi organ failure • Severe mitral or aortic valvular insufficiency or aortic dissection (VA only) • Weight >140kg • Unwitnessed cardiac arrest or CPR >60minutes
Relative Contraindications to all forms of ECMO • Trauma with multiple bleeding sites • Multiple organ failure
VV ECMO-: Absolute contraindications • Anticoagulation issues • Severe PAH • Severe Rt or Lt heart failure • Cardiac arrest
VV ECMO-: Relative contraindications • High pressure ventilation (peak insp pressure >30 cm of H2O) for >7days. • High FiO2 requirement (>0.8) for >7days • Limited vascular access. • Refusal to accept blood products
VA ECMO-: Absolute contraindications • Aortic dissection • Severe aortic valve regugitation • Anticoagulation issues
VA ECMO • Blood being drained from the venous system and returned to the arterial system. • Provides both cardiac and respiratory support. • Achieved by either peripheral or central cannulation.
VA ECMO • Decreases cardiac work • Reduces cardiac oxygen consumption • Provides adequate systemic organ perfusion with oxygenated blood. • Prevents over distension of ventricles. Helps in cardiac recovery.