Simulating ECMO.
Simulating ECMO. Andy Pybus St George Private Hospital Sydney. Conflict of interest:. MSE ( Aust ) PL www.ecmosimulation.com. Presentation plan:. Rationale for simulation. Components of a simulator. Interactive scenarios. Rationale for simulation. Why simulate? Education. Training.

Simulating ECMO.
E N D
Presentation Transcript
Simulating ECMO. Andy Pybus St George Private Hospital Sydney
Conflict of interest: MSE (Aust) PL www.ecmosimulation.com
Presentation plan: • Rationale for simulation. • Components of a simulator. • Interactive scenarios.
Rationale for simulation. Why simulate? • Education. • Training. • Competency assessment. • Therapeutic / contingency planning. • (What will happen if ??)
Components of a simulator: • Physiological models. • Pharmacological models. • Equipment models.
MyocardialContractility Chronotropy Inotropy HbDissociation ECG BloodGases MechanicalPumps CannulaFlow PKModels RespiratoryMechanics Model CO2Sensitivity BIS Baro- Reception FluidSpaces NMTransmission HypoxicResponses StarlingBehaviour V:QRelationship Vascular Pressures ThermalBehaviour
VV ECMO Paradigm: Aims: • To ‘arterialise’ as great a proportion of the venous return as is possible. • To ‘rest’ the native lung.
VA ECMO Paradigm: Aims: • Circulatory Support. • (Respiratory Support.)
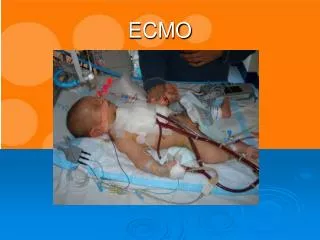
The Patient: The patient is a 24 year-old man, weighing 75 kgs, who has been admitted to your Intensive Care Unit for ongoing care. When he came in, he gave a 4 day history of increasing respiratory distress, fever and a productive cough. He deteriorated rapidly and required intubation and ventilation shortly after admission. Sputum cultures grew a sensitive staphylococcus aureus. Despite treatment with appropriate antibiotics, the use of prone ventilation, permissive hypercarbia and inhaled nitric oxide, his condition has not improved…
The clinical picture: His blood gases on 100% oxygen are: PaO2 45 mm Hg PaCO258 mm Hg pH 7.18 SaO2 74% Hb 85 g/L You calculate his Total Static Lung Compliance as: 10 ml/cm H2O You calculate his ‘Shunt’ and ‘Deadspace’ as: Qs/Qt 0.70 Vd/Vt 0.80 You estimate his oxygen consumption to be: 200 ml/min.
The clinical picture: His blood gases on 100% oxygen are: PaO245 mm Hg PaCO258 mm Hg pH 7.18 SaO2 74% Hb 85 g/L You calculate his Total Static Lung Compliance as: 10 ml/cm H2O You calculate his ‘Shunt’ and ‘Deadspace’ as: Qs/Qt0.70 Vd/Vt0.80 You estimate his oxygen consumption to be: 200 ml/min.
Subsequently… The decision is made to put the patient on VV ECMO. This is successfully implemented using a ‘Quadrox’ hollow-fibre lung and a dual-cannula drainage system. The patient is sedated, heparinised and ventilated on 70% oxygen with a PEEP of 10 cms H2O, a tidal volume of 350 mls and a rate of 8 bpm. The artificial lung is ventilated with 100% oxygen at a gas flow rate of 2.0 lpm. and ECMO blood flow rate of 3.5 lpm.
Dual drainage Cannula system: SVC drainage Atrial return IVC drainage
After 10 minutes on ECMO, you do some blood gases… PaO2: 55 mm Hg, PaCO2: 55 mm Hg You'd like to see the PCO2 a bit lower and ask your registrar what he thinks you should do. He suggests increasing the patient’s tidal volume to 600 mls and upping the rate to 15 bpm. Is this appropriate?
The clinical picture: His blood gases on 100% oxygen are: PaO245 mm Hg PaCO258 mm Hg pH 7.18 SaO2 74% Hb 85 g/L You calculate his Total Static Lung Compliance as: 10 ml/cm H2O You calculate his ‘Shunt’ and ‘Deadspace’ as: Qs/Qt0.70 Vd/Vt0.80 You estimate his oxygen consumption to be: 200 ml/min.
VV ECMO: PaCO2 and Gas Flow: Blood Flow: 5.0 lpm Blood Flow: 5.0 lpm
You also think that you'd like the patient’s SaO2a bit higher and ask your registrar what he thinks you should do. He suggests increasing the blood flow through the ECMO system. Could he be right (this time)?
You contemplate cooling the patient to 35Oc in order to further improve oxygenation. You discuss this plan with the registrar (who has a lot of experience with these kind of cases). He tells you that reducing the patient’s temperature will have no effect on his SaO2. Is he right?
ECMO and Temperature: Blood Flow: 5.0 lpm
VV ECMO: Basic Manipulations: Gas Flow Blood Flow “A simple technique for use in a complex environment.” • Adjusting Gas Flow will affect the PaCO2. • Adjusting Blood Flow will affect the PaO2. • Adjusting Temperature will affect the SvO2. Temperature (VO2)
VV ECMO: The Effect Of Gas Flow: Gas Flow Blood Flow • Gas flow is analogous to minute ventilation • PaCO2 is ≅ to 1/gas flow • PaCO2 is easily controlled • CO2 ‘Dissociation’ curve Temperature (VO2)
VV ECMO: The Effect Of Blood Flow: Gas Flow Blood Flow • PaO2 to blood flow • Blood flow as a fraction of cardiac output • Limits of achievable PaO2 • Effect of cardiac output • Effect of Hb dissociation curve Temperature (VO2)
VV ECMO: The Effect Of Temperature: Gas Flow Blood Flow As Temperature falls: • VO2↓ ↓ ↓ ↓ • SvO2↑↑ ↑↑ • PaO2↑↑ ↑↑ • Oxygenator Efficiency ↑↑↑ But: SvO2 is also importantly affected by Hct and CO. Temperature (VO2)
You’re still worried about the patient’s saturation. Your registrar tells you that further increasing the gas flow through the artificial lung will increase the SaO2. Is he right?
You’ve now been a bit worried about hypoxia all day and you notice that the patient has a haematocrit of 25% The registrar (who has a lot of experience with these kind of cases) suggests that you transfuse the patient.
The registrar (who’s now beginning to get on your nerves) also points out that the patient’s last known cardiac output was over 9 lpm. He suggests that reducing the patient’s output will increase his arterial PO2. Could he be right??
VV ECMO: The Effect of ↑ Cardiac Output: Competing influences: • PaO2tends to rise because: • As CO ↑, so SvO2↑. • As SvO2 ↑↑, so SaO2↑↑.
VV ECMO: The Effect of Cardiac Output: Competing Influences: • PaO2 tends to fall because: • As CO↑, so fraction of CO passing through the oxygenator ↓. • As CO ↑, so Qs/Qt↑.↑ Lynch JP, Mhyre JG, DantzkerDR. Influence of cardiac output on intrapulmonary shunt. J Appl Physiol. 1979 Feb;46(2):315-21.
VV ECMO: The Effect of ↑ Cardiac Output: Net Effect: As CO ↑, so PaO2↓.
You want to go home after a long day, but need to know that the registrar can change the oxygenator if he really has to. You ask him how long it will take him. He tells you “30 seconds”. You then ask him how long it will take before the patient desaturates profoundly. He tells you “Five minutes or so”… Is his confidence well-founded?
On the ward round the following day, you’re discussing the concept of ‘Resting’ the lung. The registrar asserts that: “If VV ECMO is working very well, there’s no requirement for tidal ventilation.” Could he be right?
VV ECMO: Resting the lung: PaO2 PaCO2
The registrar then goes on to say: “Even at low blood flow rates, VV ECMO can usually control arterial PCO2.” Surely, he’s not right again?
You’re now getting pretty exasperated with the registrar. He’s getting far too many answers right!! In desperation, you ask him how he thinks the patient would respond to VA ECMO. You’re not sure what size of arterial return cannula should be used. The registrar tells you a 15F cannula will be fine. Is he right?
Return (Arterial) Cannula: Basis for recommendation: ? Blood Flow: 5.0 lpm
So here I’ve started the patient on VA ECMO at a blood flow rate of over two lpm. I do a blood gas and note that the PaO2 is only ~ 70 mm Hg. The registrar tells me that the oxygenator is probably failing. Could he be right?
VA ECMO: Differential Circulation: If peripheral arterial cannulation is used, then in the ‘proximal’ circulation: • PaO2 is set by adjusting FiO2 / PEEP to native lung. • PaCO2 is set by adjusting oxygenator settings. • Requirement for tidal ventilation reduced.
VA ECMO: Special problems: • The ‘unclamped’ circuit. • Pump flow : Pre-load nexus. • Differential circulation. • Afterload dependence. • Left heart stasis. • Limb ischaemia.
Presentation available at: www.ecmosimulation.com ‘Downloads’ section.