Download
1 / 25
270 likes | 292 Vues
Management of Carotid Body Tumors. Nadir Ahmad, MD, FACS Division Head/Associate Professor of Surgery Otolaryngology-Head & Neck Surgery Cooper University Hospital & Medical School Director, Head & Neck Cancer Program MD Anderson at Cooper Cancer Center. Disclosure.

E N D
Management of Carotid Body Tumors Nadir Ahmad, MD, FACS Division Head/Associate Professor of Surgery Otolaryngology-Head & Neck Surgery Cooper University Hospital & Medical School Director, Head & Neck Cancer Program MD Anderson at Cooper Cancer Center
Disclosure No conflicts of interest to disclose
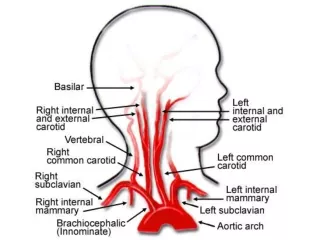
Carotid body tumors (CBT) Rare tumors (In US, 1-2 per 100,000) 60-65% of paragangilomas in H&N Overwhelmingly benign (90-95%). M:F ~1:1 Malignant CBT Not a pathologic diagnosis, nor based on aggressive behavior Presence of metastases to cervical LNs or distant sites Arise from carotid body with adventitia at medial aspect of carotid bifurcation Carotid body arises from neural crest Responds to acute fluctuations in concentrations of O2 and CO2, as well as pH Protects organs from hypoxic damage thru release of neurotransmitters that help regulate ventilator rate
Carotid Body Small, reddish-brown, oval structure in the posteromedial aspect of the bifurcation Although considered subadventitial, actual location is periadventitial Feeder vessels from ascending pharyngeal artery thru Mayer’s ligaments Innervated by Hering nerve branch of IX
Carotid body tumors (CBT) Classification Sporadic Most common (85%) Familial More common in younger pts (2nd-4th decade) More often bilateral and multiple (5% of CBT are bilateral) Gene for familial paragangliomas (PLG1) at the 11q23 locus Gene is transmitted in AD pattern with genomic imprinting Affected man has 50% chance of having affected child Affected woman will not have affected child but can pass inactivated gene to next generation Hyperplastic Arises in patients with chronic hypoxia (ie. COPD, cyanotic heart disease), including those living in high altitudes Occasionally associated with syndromes that have non-paraganglionic tumors (MEN type II, VHL, NF-1)
CBT Typically present in mid-life as asymptomatic, non-functional, lateral neck mass (soft, nontender, pulsatile) Median age of onset – 45 yrs Slow-growing (doubling time ~7 yrs, median growth of 0.83mm/yr Typically vertically fixed because of attachment to carotid bifurcation (Fontaine sign). Can have associated bruit ~10% present with CN palsy IX, X, XI, superior laryngeal nerve, sympathetic chain Sxs: pain, dysphonia, dysphagia, Horner’s syn, tongue paresis, shoulder dysfunction, FUO
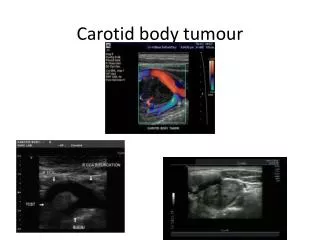
CBT - Workup Functional tumors are rare Check serum and urine catecholamines Symptoms similar to pheochromocytoma (paroxysmal HTN, palpitations, diaphoresis) CBT is an imaging diagnosis! Don’t do FNA. Initial imaging: US, color Doppler, CT with IV contrast, MR CT – splaying of ICA and ECA MRI – classic ‘salt and pepper’ appearance on T-1 weighted images ‘salt’ – slow flow or hemorrhage thru tumor ‘pepper’ – high velocity arterial branch flow voids
CBT - Workup CT angiography MR angiography Conventional angiography
CBT – Historical perspective Earliest successful resection in 1903 by Scudder Significant complications up till 1960-70s leading Hayes Martin to recommend against resecting extensive CBT (Shamblin III) Advances in imaging & surgical techniques have vastly improved safety & success of operation
CBT - Staging Shamblin classification – 3 types Type I Small localized tumor easily dissected from adjacent vessels in peri-adventitial plane Type II Larger, more adherent tumors, with partial surrounding of vessels Type III Completely surround/encase bifurcation
Pre-treatment details & counseling Factors to consider Does the tumor need to be treated at all? What is consequence of leaving tumor alone? What is the health & functional status of the patient? If considering treatment, surgery or XRT? If considering surgery, is preoperative embolization or balloon occlusion test needed? Does a vascular surgeon need to be involved? What are the potential complications from XRT or surgery? ANSWERS: Thorough understanding of the natural history/behavior of the tumor Thorough understanding of the risks of treatment as well as observation Thorough understanding of pre-treatment genetic counseling in the case of familial tumors and pre-treatment physiologic management in the case of functional tumors Thorough understanding of the surgical techniques that minimize morbidity in the event that surgery is selected by patient
Pre-treatment details & counseling MOST IMPORTANT POINT Multidisciplinary management Surgeon (Head & Neck) Surgeon (Vascular) Interventional Radiologist Radiation Oncologist Neurologist Primary care physician Speech/Swallow Therapy ENSURES THAT PATIENT HAS SOLID UNDERSTANDING OF TREATMENT OPTIONS AND POTENTIAL OUTCOMES AND RAMIFICATIONS, AND IS EMPOWERED WITH RESPECT TO THEIR CARE.
CBT - Management Observation is not recommended for most tumors as further growth & compression can ensue. However, patient preference is paramount In most centers in the US, surgery is preferred treatment modality. Surgery should be rendered in high-volume, tertiary care centers Radiation therapy is generally reserved for elderly pts, poor surgical candidates, pts with multiple paraganglia in whom surgery would be highly morbid, and in pts with recurrent tumors Highly debated Often not radiosensitive (generally goal is not cure but to slow/halt progression) Can regrow after suppression Difficult to resect after XRT due to fibrosis. Concern for XRT-induced tumors (esp in young pts), carotid artery disease, ORN
CBT - Management Surgery Ideal for tumors < 5cm & in young and/or healthy patients Difficult in larger, Shamblin type III tumors. Operative risk directly related to size & extent of tumor Most often achieved via transcervical approach Can be associated with cranial nerve palsies (classically IX, X) so preop counseling very important with contingency plan for rehab postop Must discuss other risks with patient (bleeding, infection, need for grafting, stroke, death) Preoperative embolization +/- balloon occlusion test is controversial Considered typically in Shamblin type II & III tumors to ↓ intraop bleeding Preop embolization done 48-72 hrspreop before fibrosis sets in Plethora of studies/reports do not show decrease in operative time, length of hospital stay, intraop blood loss or increase in cranial neuropathies Helpful in larger type II and all type III tumors, including balloon occlusion test ~5% risk of stroke in CBT surgery
CBT - Management Surgery For large tumors (Shamblin II & III), always involve vascular surgeon to be on standby should a bypass graft be needed. This rarely occurs but is also helpful from medico-legal perspective Bilateral tumor resection associated with greater morbidity, including risk of baroreceptor reflex failure (labile BP difficult to control medically). Staging surgery is best option, with consideration of XRT if initial surgery resulted in complications) Intraoperative details & pearls for successful operation Strong headlight illumination & loupe magnification Pre- and intra-op communication with Anesthesiologist Need good assistant! Bipolar cautery & suction (provision for 2 suction setup) Proximal & distal control of vessels Meticulous dissection in peri-adventitial plane (Plane of Gordon-Taylor) with knife or atraumatic dissecting instrument (McCabe) – helps minimize problems Postoperative admission in ICU or Stepdown Unit to monitor for postop hemorrhage or late CVA
CBT – Surgical complications Cranial neuropathy Most commonly injured CN – Superior laryngeal branch of X Vagus injury - Aspiration/dysphagia/dysphonia XI – shoulder pain/weakness; XII – tongue weakness/dysphagia; sympathetic chain – Horner’s syndrome First Bite Syndrome Disruption of sympathetic innervation to ipsilateral parotid gland Difficult to treat – NSAIDs, Neuropathic pain meds (Gabapentin, TCA, Tegretol), Botox A intraparotid injection, anticholinergics, reassurance Baroreceptor reflex failure Loss of bilateral Hering nerves Labile HTN Sympatholytics/Clonidine Stroke
Conclusions Multidisciplinary pre-treatment evaluation is paramount to treatment success Surgery remains the best treatment modality Surgeon must employ meticulous surgical technique Preoperative embolization & balloon occlusion test is controversial & can be considered in larger tumors Understanding postoperative complications is essential for patient counseling