Download

1 / 20
200 likes | 390 Vues
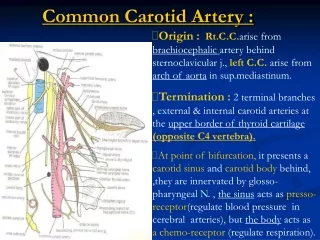
Carotid Disease. Core Surgical Trainees Vascular Teaching Day Kent and Canterbury Hospital 1st December 2009. J W B Senaratne, Cons Vasc Surgeon S J Matheiken, SpR Vasc Surgery. Why talk about it?. Stroke is the third leading cause of death

E N D
Carotid Disease Core Surgical Trainees Vascular Teaching Day Kent and Canterbury Hospital 1st December 2009 J W B Senaratne, Cons Vasc Surgeon S J Matheiken, SpR Vasc Surgery
Why talk about it? • Stroke is the third leading cause of death • A third of patients who stroke will do so again within 5 years • Some strokes are preventable
And what should we talk about? • CEA • CAS • BMT
UNMODIFIABLE Age Gender Previous CVA Family history CVA MODIFIABLE Smoking Blood Pressure Diabetes Mellitus Hyperlipidaemia Carotid stenosis Risk Factors for Stroke
Relevant CEA trials • Joint study of extracranial arterial occlusion • NASCET • ECST • ACAS • ACST
What should the patient know? • What are the benefits of having a carotid endarterectomy • What are the risks involved?
Complications of CEA • Stroke / Mortality : 1 – 3 % • Cranial Nerve injury: • Haemorrhage • Restenosis • Paraesthesiae
Indications for CEA • NNT to prevent major stroke/ death • At 5 years: • Medical group: 25% stroke / death • CEA group: 15% stroke / death • ARR: 10% • RR reduction: 40% • NNT: 10 • These numbers are for sympatomatic patients with critical stenosis of the ICA
Incidentally detected asymptomatic ICA stenosis and you • ACAS: 3 year outcome 11% in medical group vs 5.1% in CEA : • NNT 17 with complication rate under 3%
CETC findings • Symptomatic stenosis over 50% benefits from prompt intervention • Benefit is higher in severe disease 70-99% • Maximum benefit if intervention within 2-4 week of symptoms • No benefit for intervention beyond 12 weeks in 50-69% disease • No benefit for intervention beyond 4 weeksin women with 50-69% stenosis • No benefit for intervention inasymptomatic women
Timing of CEA • Half the preventable strokes after a TIA or initial stroke occur within 7 days
Indications for CEA in EKHT • RACE • Acute symptoms wih stenosis 50 – 99% • TIA with ABCD2 score 4-6 • ASA 1 or 2 • Elective CEA • Symptomatic stenosis 50-99% • Stroke in prev 6/12, TIA, AmFugax, Tinnitus • Asymptomatic stenosis 60-99%, not F > 70y
Carotid Stenting • Leicester, LEXINGTON, WALLSTENT • CAVATAS – UK/ Europe • EVA-3S - France • SPACE – Germany / Austria • ICSS – Europe • CREST – North America
Outcomes of asymptomatic CAS trials • SPACE – no statistical difference 30-day • EVA-3S: stopped twice due to stroke rates • CAVATAS – comparable results but high restenosis • SAPPHIRE – comparable results, but interpretation bias, stopped early
Conclusions from CAS evidence • High death / stroke rates for CAS in elderly (over 80 in CREST; over 75 in SPACE) • No evidence in favour of CAS in symptomatic patients not high risk for CEA; should be done as part of trial • CAS an acceptable alternative when pt high risk for CEA, especially recently symptomatic, male, <75y • No evidence that CAS has any benefit over BMT in the asymptomatic patient whether high risk or not for CEA and not recommended unless IAPR <4%.
BMT • Lag-phase for effect • More important in asymptomatic group • Based on ACST BMT data, 1000 interventions at 30 day rate 2.8% would prevented only 53 strokes
Things to clarify • Quantification of disease in trials • Reccos for asymptomatic disease; risk reductions • Incidence of other complications in CEA
Take Home Messages • Symptomatic stenosis over 70%: must intervene as soon as safely possible • Symptomatic stenosis 50-69%: consider for intervention on individual basis • Asymptomatic stenosis: intervention on individual basis • CEA vs stenting: ongoing trials; CEA preferred in most settings; CAS acceptable in symptomatic stenosis in patient at high risk for CEA procedure.