Download
1 / 34
350 likes | 1.29k Vues
Carotid, Subclavian, and Vertebrobasilar Disease. Kelley Hodgkiss-Harlow 9/30/2009. Carotid Disease: History. 1875—Gowers case report of R hemiplegia/L blindness 1914—Hunt recognizes syndrome of TIAs as prodrome to stroke 1937—Moniz: Arteriography used to diagnose carotid artery occlusion

E N D
Carotid, Subclavian, and Vertebrobasilar Disease Kelley Hodgkiss-Harlow 9/30/2009
Carotid Disease: History • 1875—Gowers case report of R hemiplegia/L blindness • 1914—Hunt recognizes syndrome of TIAs as prodrome to stroke • 1937—Moniz: Arteriography used to diagnose carotid artery occlusion • 1954—Eastcott publishes first report of successful CEA
Pathology • Atherosclerosis: 90% • Deposition fat intimafatty plaque with intermittent hemorrhage/ulceration • Bifurcation predominance-secondary to arterial geometry, velocity profile, and wall shear stress • Other 10%: • FMD • Mechanical • Inflammatory • Radiation
Stroke • 3rd leading cause of death in USA • Age is risk factor: • Male:female ratio about 1.5:1 • >65 y/o incidence 150-200/100,000 • High rate of recurrence if no intervention: • 10-20% within one year, 20-42% within 5 years • Roughly accepted 10%/yr recurrence risk • Majority recur within one year • High mortality rate with recurrence • 35-65%
Stroke distribution • MCA: contralateral sensory/motor loss, head and eye deviation toward infarcted side • left—aphasia/neuropsych symptoms • ACA: rare, contralateral lower extremity weakness/sensory, urinary incont, apathy, mutism, gait apraxia • PCA: mesencephalon, thalamus, occiptal and temporal lobes—homonymous visual field deficit, alexia, prosopagnosia, amnesia, hallucinations • Watershed areas: ACA/MCA and MCA/PCA borders • Lacunar (brain stem, basal ganglia): pure motor, pure sensory, ataxis hemiparesis, and dysarthria.
TIA • Definition: Transient focal neurologic deficit of either anterior or posterior circulation • Rochester study: TIAs followed for five yr • Incidence stroke 36% • 51% of these occurred within first year • Lit review: annual stroke incidence in pts with TIAs ranges from 5.3-8.6%/yr for first 5 years • Approx 1/3 pts with TIA will suffer stroke within 5 years
TIA II • Embolic theory of transient cerebral ischemia (versus mechanical flow reduction) • Atheromatous debris, thrombus, or plt aggregates • Ischemic attacks stop after occlusion • TIA vs small stroke? Cerebral infarction and atrophy is correlated with percent stenosis and h/o TIAs • 2% e/o stroke on CT with pts with ‘mild’ stenoses • 58% in pts with asymptomatic high-grade stenoses • Therefore, important to identify asymptomatic lesions BEFORE TIA occurs
Timing of CEA • Historically: weeks to months delay after TIA or stroke • ipsilateral hemorrhage and extension of the infarct supported in several series • Old data prior to current imaging studies • No RCT addressing the question • Large meta-analysis 2003: • No diff between rates of stroke or death for pts with stable stroke symptoms when CEA performed early (<3-6 weeks) or delayed (>3-6 weeks) • Pooled analysis of NASCET and ESCT data • Greatest benefit from surgery in group randomized within 2 wks of surgery and this benefit decreased with further delay from symptom onset
Imaging Studies • CT scan—90% cortical ischemic infarctions are detectable with a clinical neurologic event after 24h • Hypodensities, mass effects, loss of distinction between cortical gray and subcortical white matter • Hemorrhagic areas of reperfusion • Only dx ~50% brainstem infarcts • CTA vs. Angiography: Overal accuracy for correct stenosis 90-96%, risks of complications avoided • MRA: Sensitivity 83-97% and specificity 92-98% for detecting flow voids, tends to overestimate when compared to angiography
Symptomatic Disease • NASCET:2226 pts randomized to medical care or CEA. • Patients had either a transient ischemic attack or stroke within 4 months of enrollment and a 30-99% internal carotid artery stenosis. • For patients with a >=70% stenosis, carotid endarterectomy reduced the risk of any ipsilateral stroke from 26% to 9% at 2 years (P<0.001). • Conclusion: CEA better if symptomatic with stenosis >70%
Asymptomatic disease • Natural history studies: 30-50% pts who have suffered a stroke did NOT have TIA prior • 20% pts with bruit will have hemodynamically significant stenosis of the carotid bulb • ACAS trial (1995): Called off after 2.7 yrs f/u • 5 yr risk for ipsi stroke, any periop stroke, and death was 5.1% surgical group c/w 11% medical group. • Absolute risk reduction of 5.9% and relative risk reduction of 53% in favor of CEA. • Combined neurologic morbidity and mortality 1.52% for surgery.
Asymptomatic Disease II • Conclusion: CEA better if can offer with morbidity/mortality <1.5%, recc if >60% stenosis • Corresponds to 80% stenosis when using standardized duplex criteria • ASCT (2004): 5 yr trial results confirm and extend ACAS results. • 5 yr risk for ipsi stroke, any periop stroke, and death was 6.4% surgical group c/w 11.8% medical group. • Benefit in pts >60% stenosis • Most benefit in pts >75 y/o
Duplex Criteria • Individualized to each vascular laboratory with a program of internal quality control.
Pre-Op Medications • Antiplatelet Therapy • Cochrane meta-analysis: ASA 81mg statistically significant benefit in reducing rate of stroke from any cause, but not death or cardiac events • 81mg as effective as 325mg with less bleeding complications/risks • Statin • Reduction in in-hospital mortality, perioperative stroke and death rates, but not in-hospital cardiac events • Multivariate analysis: 3-fold reduction in stroke, 5-fold reduction in death
CEA: Techniques • Vertical vs. Horizontal Incision • Identification and Mobilization: • Cervical lymph nodes • Hypoglossal nerve • Gaining distal ICA exposure: • Digastric muscle division • Mandibular subluxation • Endarterectomy—Eversion vs. Patch • No difference in rate of stroke/death • Advantage—faster, less exposure, no suture line on ICA • Disadvantage—tech challenging, mobilization of bulb, less visualization of endpoint, shunting cumbersome • Shunting—”snow plowing the intima”
Selective Shunting • Local/Regional Anesthesia (0-1.1% permanent deficit) • 10% all procedures done • Lesser fluctuations in blood pressure • EEG Monitoring (1.5-3.5%) • Wide threshold between EEG monitoring becoming abnormal vs. infarction • ?sensitivity/specificity • Stump pressure measurements (0.8-2%) • 50mmHg based on correlations with EEG monitoring, status of contralateral artery, and reported outcomes
To Shunt or Not To Shunt • Clamping ischemia is uncommon cause of perioperative stroke • 93-96% pts tolerate carotid clamping without shunt under local/regional anesthesia • Embolization or thrombosis usually due to technical difficulties • Shunt does not protect or contribute to stroke risk—no superiority in either technique between selective shunting vs. routine shunting. (Cochrane stroke group)
Intraoperative Assessment • Operative Arteriography • If routinely performed, a reduction in mortality, stroke rate, and fatal strokes has been noted in several studies • Angioscopy • Direct visualization of the luminal surface • Increases cross-clamp time, no info on patterns of blood flow • Duplex Ultrasonography • Detection and correction of turbulent blood flow and anatomic defects lead to decreased occlusions and restenosis
CEA vs. CAS • Randomized clinical trials to gain evidence on which to base clinical decisions. • CAS vs. CEAneed to enhance our understanding of their roles. • CAVATAS—angioplasty alone vs. surgery, horrible results both arms, of historical interest only
SAPPHIRE (Stenting and Angioplasty with Protection in Pts at High Risk for Endarterectomy) • Initially, data showed results for stenting statistically significantly superior to those of CEA….but • Primary endpoint was amalgam of short and intermediate term results (periprocedural stroke, MI, or death, and one year ipsilateral stroke or death) • No statistically significant difference in outcome in any individual endpoint (death, stroke, or MI). • Majority of MI’s were non Q-wave and of doubtful significance. • <30% high-risk pts had symptomatic dz, treatment groups are not equal in terms of comorbidities/age • No medical management arm
Symptomatic Trials • EVA-3S: >60% symptomatic stenosis equally eligible pts • 30 day: Stroke/death rates 3.9% (CEA) vs. 9.6% (CAS) • 6 months: 6.1% vs. 11.7% • But…less experienced surgeons, no CPD • SPACE: symptomatic pts randomized CEA vs. CAS, failed to prove “non-inferiority” • CPD in only 27%
CREST • 2500 pts equally eligible for CEA vs. CAS, enrolled based on NASCET/ACAS guidelines (50%/70%) • Lead-in results suggest that older pts suffer worse outcomes (P=0.0006)
Conclusions: CAS vs. CEA • The low morbidity and mortality rates in both nonrandomized and randomized series studying CEA for both asymptomatic and symptomatic pts must be equaled for CAS. • 30d stroke and stroke/mortality rates for CAS appear to be marginally statistically significantly higher than those associated with CEA (1.3%) • Accepted indications: • Surgically inaccessible lesion • Hostile Neck • Restenosis • Medical high risk (hard to define) • Participation in RCT
Vertebrobasilar Ischemia • Symptoms: Commonly manifested as vertigo, visual disturbances, progressive neuro deficit • Mechanisms: • Microembolization: from heart or more proximal arteries. Less common. • innominate, prox subclavian, and vertebrals • Low-flow: lack appropriate inflow from the vertebral artery and have inadequate compensation from the carotid. • More frequent • Stenosis/occlusion of vert, also extrinsic compression • Orthostatic hypotension, antihypertensive meds, arrythmias, CHF, pacemaker malfunction, anemia
Evaluation of Patients • Dizziness, vertebral artery stenosis are common complaints/findings • Imaging brain to r/o tumor, investigate for infarctions • Check bilateral arm BP’s to r/o subclavian steal syndrome • Document reversal of flow by duplex • Extrinsic compression by osteophytes • Turning head side to side, slowly, then briskly to differentiate from BPV • Confirm with angiogram
Global ischemia • “Drop attacks” comprise roughly 30% of presentations • One or both internal carotid arteries occluded or with severe siphon stenosis. • Vertebral arteries important pathways for cerebral revascularization when they are critically stenosed or occluded. • Minimal anatomic req to justify vert reconstruction is >60% stenosis in dominant if contra is hypoplastic, or >60% in both.
Angiography • Most common athersclerotic lesion is stenosis of its origin • Presence of post-stenotic dilation proximally is suggestive of hidden stenosis • Extrinsic compression seen at V2—multiple views/manipulation necessary • V2-V3 segments: site of traumatic injury from periosteum/adventitia fixation • V3 usually area of reconstitution secondary to collaterals from occipital artery
Treatment • Anticoagulation • Trial of medical therapy prior to pursuing any surgical intervention • Most effective for lesions that cause symptoms through embolization or thrombosis of small arteries • If definite clinical syndrome, MRI documenting absence of alternate pathology, arteriography with structural lesion, and persistent symptoms on anticoagulationsurgery
Surgical Options • Transposition of Vertebral Artery into the Common Carotid Artery • Origin stenosis • Supraclavicular at level of C6 • Patency 90-97%, stroke risk 2%, mortality risk <1% • Complications: Horner’s, lymphocele • Distal Vertebral Artery Reconstruction • GSV • Level of C2 • Endovascular interventions?
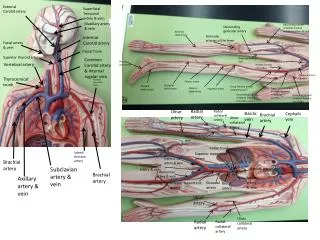
Subclavian Disease • Atherosclerotic disease left>right • Asymptomatic lesions even with asymptomatic stealtreatment deferred • Subclavian steal: • Retrograde blood flow associated with proximal subclavian stenosis or occlusion • Upper extremity ischemia (71%), VBI (44%), Hemispheric TIA (29%)
Subclavian Steal Syndrome • Physical exam • Blood pressure differential >=20mmHg • 2-3x more common on the left • Embolic phenoma to hands • Duplex ultrasonography • Reversal blood flow within vertebral • Monophasic waveforms in subclavian a. • High-frequency blood flow pattern • Arch aortography with selected views
Treatment • Treat ICA lesion first! • If symptoms persist • Transposition of subclavian artery onto the common carotid • Approx 100% patency rate at followup • Carotid-Subclavian bypass • Approx 94% patency at 10 years • Axilloaxillary bypass • Setting of previous extensive neck surgery or radiation • Long-term durability inferior • Subclavian artery stenting/angioplasty