Download
1 / 113
1.14k likes | 1.25k Vues
Explore the intricate world of hemodynamic disorders, thromboembolic disease, and shock. Learn about edema and its causes, such as increased hydrostatic pressure, reduced oncotic pressure, lymphatic obstruction, and sodium/water retention. Discover the role of water in the body and the various types of edema. Delve into the complexities of hyperemia, congestion, hemorrhage, hemostasis, thrombosis, embolism, infarction, and shock.

E N D
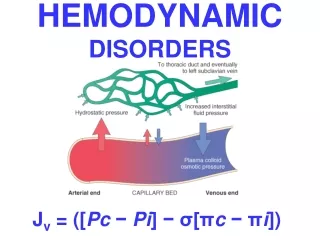
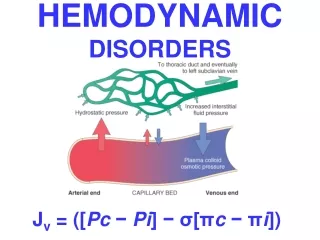
HEMODYNAMIC DISORDERS Jv = ([Pc − Pi] − σ[πc − πi])
Hemodynamic Disorders • Thromboembolic Disease • Shock
Overview • Edema (increased fluid in the ECF) • Hyperemia (INCREASED flow) • Congestion (INCREASED backup) • Hemorrhage (extravasation) • Hemostasis (opposite of thrombosis) • Thrombosis (clotting blood) • Embolism (downstream travel of a clot) • Infarction (death of tissues w/o blood) • Shock (circulatory failure/collapse)
EDEMA • ONLY 4 POSSIBILITIES!!! • Increased Hydrostatic Pressure • Reduced Oncotic Pressure • Lymphatic Obstruction • Sodium/Water Retention
WATER • 60% of body • 2/3 of body water is INTRA-cellular • The rest is INTERSTITIAL • Only 5% is INTRA-vascular • EDEMA is SHIFT to the INTERSTITIAL SPACE • HYDRO- • -THORAX, -PERICARDIUM, -PERITONEAL • EFFUSIONS, ASCITES, ANASARCA
INCREASED HYDROSTATIC PRESSURE • Impaired venous return • Congestive heart failure • Constrictive pericarditis • Ascites (liver cirrhosis) • Venous obstruction or compression • Thrombosis • External pressure (e.g., mass) • Lower extremity inactivity with prolonged dependency • Arteriolar dilation • Heat • Neurohumoral dysregulation
REDUCED PLASMA ONCOTICPRESSURE (HYPOPROTEINEMIA) • Protein-losing glomerulopathies (nephrotic syndrome) • Liver cirrhosis (ascites) • Malnutrition • Protein-losing gastroenteropathy
LYMPHATIC OBSTRUCTION(LYMPHEDEMA) • Inflammatory • Neoplastic • Postsurgical • Postirradiation
Na+ RETENTION • Excessive salt intake with renal insufficiency • Increased tubular reabsorption of sodium • Renal hypoperfusion Increased renin-angiotensin-aldosterone secretion
INFLAMMATION • Acute inflammation • Chronic inflammation • Angiogenesis
CHF EDEMA • INCREASED VENOUS PRESSURE DUE TO FAILURE • DECREASED RENAL PERFUSION, triggering of RENIN-ANGIOTENSION-ALDOSTERONE complex, resulting ultimately in SODIUM RETENTION
HEPATIC ASCITES • PORTAL HYPERTENSION • HYPOALBUMINEMIA
RENAL EDEMA • SODIUM RETENTION • PROTEIN LOSING GLOMERULOPATHIES (NEPHROTIC SYNDROME)
EDEMA • SUBCUTANEOUS (“PITTING”) • “DEPENDENT” • ANASARCA • LEFT vs RIGHT HEART • PERIORBITAL • PULMONARY • CEREBRAL (closed cavity, no expansion) • HERNIATION of cerebellar tonsils • HERNIATION of hippocampal uncus over tentorium • HERNIATION, subfalcine
Transudate vs Exudate • Transudate • results from disturbance of Starling forces • specific gravity < 1.012 • protein content < 3 g/dl, LDH LOW • Exudate • results from damage to the capillary wall • specific gravity > 1.012 • protein content > 3 g/dl, LDH HIGH
HYPEREMIA Active Process CONGESTION Passive Process Acute or Chronic
CONGESTION • LUNG • ACUTE • CHRONIC • LIVER • ACUTE • CHRONIC • CEREBRAL
Kerley B Air Bronch-ogram
HEMORRHAGE • EXTRAVASATION beyond vessel • “HEMORRHAGIC DIATHESIS” • HEMATOMA (implies MASS effect) • “DISSECTION” • PETECHIAE (1-2mm) (PLATELETS) • PURPURA <1cm • ECCHYMOSES >1cm (BRUISE) • HEMO-: -thorax, -pericardium, -peritoneum, HEMARTHROSIS • ACUTE, CHRONIC
EVOLUTION of HEMORRHAGE • ACUTE CHRONIC • PURPLE GREEN BROWN • HGB BILIRUBIN HEMOSIDERIN
HEMOSTASIS • OPPOSITE of THROMBOSIS • PRESERVE LIQUIDITY OF BLOOD • “PLUG” sites of vascular injury • THREE COMPONENTS • VASCULAR WALL, i.e., endoth/ECM • PLATELETS • COAGULATION CASCADE
SEQUENCE of EVENTSfollowing VASCULAR INJURY • ARTERIOLAR VASOCONSTRICTION • Reflex Neurogenic • Endothelin, from endothelial cells • THROMBOGENIC ECM at injury site • Adhere and activate platelets • Platelet aggregation (1˚ HEMOSTASIS) • TISSUE FACTOR released by endothelium, plats. • Activates coagulation cascadethrombinfibrin (2˚ HEMOSTASIS) • FIBRIN polymerizes, TPA limits plug
PLAYERS • ENDOTHELIUM • PLATELETS • COAGULATION “CASCADE”
ENDOTHELIUM • NORMALLY • ANTIPLATELET PROPERTIES • ANTICOAGULANT PROPERTIES • FIBRINOLYTIC PROPERTIES • IN INJURY • PRO-COAGULANT PROPERTIES
ENDOTHELIUM • ANTI-Platelet PROPERTIES • Protection from the subendothelial ECM • Degrades ADP (inhib. Aggregation) • ANTI-Coagulant PROPERTIES • Membrane HEPARIN-like molecules • Makes THROMBOMODULIN Protein-C • TISSUE FACTOR PATHWAY INHIBITOR • FIBRINOLYTIC PROPERTIES (TPA)
ENDOTHELIUM • PROTHROMBOTIC PROPERTIES • Makes vWF, which binds PlatsColl • Makes TISSUE FACTOR (with plats) • Makes Plasminogen inhibitors
ENDOTHELIUM • ACTIVATED by INFECTIOUSAGENTS • ACTIVATED by HEMODYNAMICS • ACTIVATED by PLASMA • ACTIVATED by ANYTHING which disrupts it
PLATELETS • ALPHA GRANULES • Fibrinogen • Fibronectin • Factor-V, Factor-VIII • Platelet factor 4, TGF-beta • DELTA GRANULES (DENSE BODIES) • ADP/ATP, Ca+, Histamine, Serotonin, Epineph. • With endothelium, form TISSUE FACTOR
NORMAL platelet on LEFT, “DEGRANULATING” ALPHA GRANULE ON RIGHT AT OPEN WHITE ARROW