Chapter 2 Inflammation and Repair
1.57k likes | 2.49k Vues
Chapter 2 Inflammation and Repair. Outline Injury Natural (Innate) Defenses Against Injury Inflammation Regeneration and Repair Injuries to Teeth Injuries to Soft Tissues Reactive Connective Tissue Hyperplasia Inflammatory Periapical Lesions. Inflammation and Repair. (pg. 34)

Chapter 2 Inflammation and Repair
E N D
Presentation Transcript
Chapter 2 Inflammation and Repair
Outline Injury Natural (Innate) Defenses Against Injury Inflammation Regeneration and Repair Injuries to Teeth Injuries to Soft Tissues Reactive Connective Tissue Hyperplasia Inflammatory Periapical Lesions
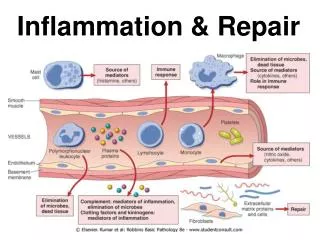
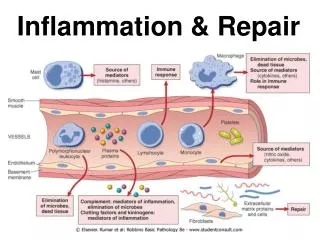
Inflammation and Repair (pg. 34) The body’s response to injury Inflammation Allows the body to eliminated injurious agents, contain injuries, and heal defects
Injury (pg. 34) An alteration in the environment that causes tissue damage Examples include Physical Chemical Microorganisms Nutritional deficiencies
Natural (Innate) Defenses Against Injury (pg. 34) Intact skin or mucosa is a physical barrier. Enzymes in saliva have an antibacterial activity. Flushing action of tears, saliva, urine, and diarrhea removes foreign substances.
Inflammation (pgs. 34-44) Microscopic Events and Clinical Signs of Inflammation White Blood Cells and Their Involvement in the Inflammatory Response Biochemical Mediators of Inflammation Systemic Manifestations of Inflammation Chronic Inflammation Hyperplasia, Hypertrophy, and Atrophy
Inflammation (cont.) (pgs. 34-35) A nonspecific response to injury Occurs in the same manner regardless of the nature of the injury May be local and limited to the area of injury, or may be extensive if the injury is extensive May be acute or chronic
Microscopic Events and Clinical Signs of Inflammation (Cont.)
Microscopic Events and Clinical Signs of Inflammation (Cont.) (pgs. 35-37) (Table 2-1) Local clinical changes are classic signs of inflammation. Redness, heat, swelling, pain, loss of normal tissue function Systemic signs may include Increase in body temperature Increase in the number of white blood cells Enlargement of lymph nodes
Microscopic Events and Clinical Signs of Inflammation (cont.)
Microscopic events involve microcirculation. Arterioles, capillaries, venules in the area of injury White blood cells Chemical mediators Usually, an exchange of oxygen and nutrition is seen in these vessels. Most of the fluid reenters circulation through venules. Lymphatic system carries away fluid that does not reenter the blood vessels. Microscopic Events and Clinical Signs of Inflammation (cont.)
Sequence of Microscopic Events (pg. 36) Injury to tissue Constriction of microcirculation Dilation of microcirculation Increase in permeability Exudate leaves microcirculation. Increased blood viscosity Decreased blood flow Margination and pavementing of white blood cells (WBCs) WBCs enter tissue. WBCs ingest foreign material.
Sequence of Microscopic Events (cont.) (pg. 36) Hyperemia Increased blood flow in capillary beds of injured tissue Will produce redness and heat Exudate Increased blood plasma and proteins in injured tissue Helps dilute injurious agents, but results in excess fluid in tissues – edema Serous exudate Mainly plasma fluids and proteins, few WBCs Purulent exudate (suppuration) Contains plasma fluids and proteins, tissue debris, and many WBCs
Sequence of Microscopic Events (cont.) (pgs. 36-38) Swelling develops as exudate escapes into tissue. May flow out as a thin, clear exudate (serous) or a thick white-to-yellow pus (purulent) Drainage may occur through a fistula. Incision and drainage (I & D) may be required. A drainage tube may be placed. Medication may be administered to treat infection and reduce inflammation. Pressure from exudate and chemical mediators may cause pain. Blood viscosity may increase due to loss of plasma fluids. Margination White blood cells migrate to the periphery of the vessel.
Sequence of Microscopic Events (cont.) (pgs. 37, 39) Emigration The process by which WBCs escape from blood vessels through gaps in endothelial cells Chemotaxis Directed movement of WBCs toward the site of injury Phagocytosis The process by which WBCs ingest and then digest foreign substances. May include pathogenic organisms and tissue debris
(pgs. 37, 39) There are six different kinds of WBCs. Neutrophils First to arrive at the site of injury Primary cell in acute inflammation Monocytes (Macrophage) Second cell in inflammatory response Lymphocytes and Plasma Cells Seen in chronic inflammation and the immune response Eosinophils and Mast Cells Seen in both inflammation and the immune response White Blood Cells and Their Involvement in the Inflammatory Response
White Blood Cells and Their Involvement in the Inflammatory Response (cont.) (pgs. 39-40) Changes occur in the proportion of WBCs as the inflammatory response continues. The neutrophil is the most common inflammatory cell in acute monocyte (in blood) becomes a macrophage as it enters tissue inflammation. The circulating. Neutrophils decrease in number. Macrophages, lymphocytes, and plasma cells become predominant with chronic inflammation.
White Blood Cells and Their Involvement in the Inflammatory Response (cont.)
White Blood Cells and Their Involvement in the Inflammatory Response (cont.)
Neutrophils (PMNs) (pgs. 39-40) 60% to 70% of WBC population Granular leukocytes along with basophils and eosinophils Derived from stem cells in bone marrow Contain lysosomal enzymes Function is phagocytosis and then enzymatic destruction of foreign substances. Neutrophils then perish. The enzymes can leak, causing further tissue damage.
Macrophages (pgs. 40-41) 3% to 8% of WBC population Derived from stem cells in bone marrow Has a single, round nucleus and a nongranular cytoplasm Responds to chemotactic factors, is mobile, can phagocytize – also plays a role in the immune system
Biochemical Mediators of Inflammation (pgs. 40-41) Cause many of the events in the inflammatory response Basic mediators can recruit other mediators and immune mechanisms. May be derived from Blood Endothelial cells White blood cells and platelets Pathogenic organisms as they injure the tissue
Biochemical Mediators of Inflammation (cont.) (pgs. 40-41) Three interrelated systems Interaction takes place during activation, among their products, and within their various actions Kinin system Clotting mechanism Complement system
Kinin System (pg. 40) Active in early phases of inflammation Activated by substances in plasma and injured tissue Causes increased Dilation of blood vessels at the site of injury Permeability of local blood vessels Induces pain
Clotting Mechanism (pg. 41) Clots blood and mediates inflammation Some of the clotting mechanisms products that are activated during tissue injury cause local vascular dilation and permeability by activating kinin.
Complement System (pg. 41) Involves the production of a sequential cascade of plasma proteins They are present in blood in an inactive form. A trigger (usually an antibody/antigen complex) initiates the sequence of steps. These plasma proteins function in inflammation and immunity. Some components cause WBCs known as mast cells to release histamine. Histamine causes an increase in vascular permeability and vasodilation. Other components cause cell death, form chemotactic factors for WBCs, and enhance phagocytosis.
Other Biochemical Mediators of Inflammation (pg. 41) Released by the body Prostaglandins Cause increased vascular dilation and permeability, tissue pain and redness, and changes in connective tissue Lysosomal enzymes Act as chemotactic factors May cause damage to connective tissues and to the clot
Other Biochemical Mediators of Inflammation (cont.) (pg. 41) Released by pathogenic microorganisms Endotoxin Produced by cell walls of gram-negative bacteria Serves as chemotactic factor, can activate complement, function as an antigen, and damage bone and tissue Lysosomal enzymes Have a similar chemical composition and action as those released by WBCs
Antiinflammatory Drugs (pg. 41) Block or suppress the inflammatory response Prevent or reduce clinical signs of inflammation and adverse reactions to the injury Examples Nonsteroidal antiinflammatory agents Aspirin, ibuprofen, celecoxib Steroidal antiinflammatory drug Prednisone
Systemic Manifestations of Inflammation (pgs. 41-42) May include Fever Leukocytosis Elevated C-reactive protein Lymphadenopathy
Fever (pg. 42) Controlled by the hypothalamus Associated with systemic inflammatory response Pyrogens Fever producing substances produced by WBCs and pathogens Pyrogens act on the hypothalamus. The hypothalamus increases body temperature by way of prostaglandins.
Leukocytosis (pg. 42) A systemic inflammatory response can increase the number of WBCs from the normal 4000 to 10,000/mm of blood to 10,000 to 30,000/mm. The primary cell involved is the neutrophil. The rate of formation is increased and immature forms are released from bone marrow into the blood. The body is attempting to produce more cells for phagocytosis.
Elevated C-Reactive Protein (pg. 42) C-reactive protein is produced in the liver and plays the important role of interacting with the complement system. Elevated levels are present during episodes of acute inflammation or infection. May continue with chronic inflammation Levels can be used to help assess rheumatoid arthritis and systemic lupus erythematosus. A chronic increased level is associated with an increased risk for cardiovascular disease.
Lymphadenopathy (pgs. 42-43) Enlarged and palpable superficial lymph nodes Follows route of lymphatic drainage The enlarged nodes occur due to changes in lymphocytes, which are the primary cells of the immune response. Hyperplasia An increase in the number of cells Hypertrophy Enlargement of individual cells
Chronic Inflammation (pgs. 42-43) Due to persistent injuries Cells involved include macrophages, lymphocytes, and plasma cells as well as neutrophils and monocytes present in acute inflammation. May include proliferation of fibroblasts and formation of granulomas
Chronic Inflammation (cont.) (pgs. 42-43) Granuloma Microscopic groupings of macrophages surrounded by lymphocytes and plasma cells Usually contain multinucleated giant cells Large macrophages with multiple nuclei Associated with foreign body reactions and some infections such as tuberculosis
Hyperplasia, Hypertrophy, and Atrophy (pgs. 43-44) Hyperplasia An increase in the number of cells often in response to chronic irritation or abrasion May return to normal if the insult subsides, or may persist following removal of the irritant Hypertrophy An increase in the size of cells May be seen in cardiac muscle as a response to hypertension Atrophy A decrease in size or function of a cell, tissue, organ, or entire body
Regeneration and Repair (pgs. 44-46) Microscopic Events That Occur During Repair Types of Repair Bone Tissue Repair
(pg. 44) Regeneration If the inflamed area returns to normal structure and function Repair Occurs when the damage is too great for the tissue to return to normal Functioning cells and tissue often are replaced with nonfunctioning scar tissue. Regeneration and Repair (cont.)
Microscopic Events That Occur During Repair (pgs. 44-45) Takes about 2 weeks Occurs almost simultaneously in both epithelium and connective tissue
Day of Injury (pg. 45) Blood flows into injured tissue to produce a clot. The clot contains fibrin, clumped red blood cells (RBCs), and platelets.
One Day After Injury (pg. 45) Neutrophils migrate from the microcirculation into injured tissue in an acute inflammatory response. They phagocytize foreign material and necrotic tissue.