Download
1 / 63
640 likes | 756 Vues
Explore the concepts of inflammation, tissue repair, and complications, along with specific conditions like sinusitis, burns, and rheumatoid arthritis. Learn about the pathophysiology, clinical manifestations, diagnostic criteria, and treatment options for these conditions.

E N D
Applied Pathophysiology:A Conceptual ApproachChapter 3: Inflammation and Tissue Repair
Lines of Defense • First: Skin and mucous membranes • Second: Inflammatory response • Third: Immune response
Acute Inflammation • Triggered by tissue injury • Goals of inflammation • Increase blood flow to site • Increase healing cells at site • Prepare for tissue repair
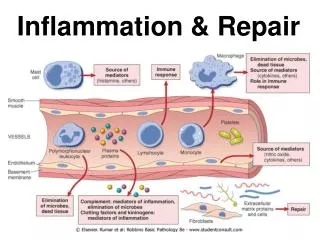
Vascular Response • Facilitated by chemical mediators • Induces vasodilation and increases capillary permeability • Objective is to get more blood flowing to the injured area
Inflammatory Mediators • Cell-derived • White blood cells • Platelets • Endothelial or damaged tissue cells • Plasma-derived • Complement system • Kinin system • Clotting system
Cellular Response • Chemotaxis • Cellular adherence • Cellular migration
Manifestations of Inflammation • Local manifestations include heat, incapacitation, pain, edema, redness • Systemic manifestations may include fever and increased circulating leukocytes and plasma proteins
Treatment of Inflammation • Reduce blood flow • Decrease swelling • Block the action of chemical mediators • Decrease pain
Healing and Tissue Repair • Inflammatory phase • Acute inflammatory response • Seal the wound • Proliferative phase • Clear the debris • Restore structural integrity • Remodeling phase • Restore functional integrity • Remodeling
Complications of Healing • Infection • Ulceration • Dehiscence • Keloids • Adhesions
Chronic Inflammation • Recurrent or persistent inflammation lasting several weeks or longer • Monocytes, macrophages, and lymphocytes more prominently involved • Formation of granulomas and scarring often occur
Application of the Concepts of Inflammation • Sinusitis • Burns • Rheumatoid arthritis (RA) • Gastritis • Pancreatitis • Inflammatory bowel disease (IBS)
Acute and Chronic Sinusitis • Pathophysiology • Clinical manifestations • Diagnostic criteria • Treatment
Acute SinusitisPathophysiology • Blockage of ostia and outflow of mucus due to allergy, viruses, or other irritants • Impaired clearance of mucus by cilia • Altered mucus quality or quantity • Cystic fibrosis
Acute SinusitisClinical Manifestations • Facial pain over sinus regions of face increasing with straining or bending down • Fever • Nasal congestion and/or excessive nasal discharge and postnasal drainage • Persistent cough • Fatigue
Acute SinusitisDiagnostic Criteria • Physical examination • General laboratory tests • Erythrocyte sedimentation rate (ESR) • C-reactive protein (CRP) test • White blood cell (WBC) count • Sinus radiographs
Acute Sinusitis Treatment • Pharmacologic • Antibiotics • Antihistamines • Decongestants • Nasal sprays • Surgical
Chronic Sinusitis Pathophysiology • Multifactorial • Environmental factors • Persistent infection • Allergens • Genetic factors • Metabolic abnormalities • Immune deficiencies • Disruption of mucociliary clearance
Chronic SinusitisClinical Manifestations • Nasal congestion • Nasal and postnasal discharge • Sore throat • Foul breath, unpleasant taste • Low-grade fever • Fatigue, anorexia • Chronic cough • Hyposmia (reduced ability to smell) • Facial fullness, discomfort, pain, and headache (with polyps)
Chronic SinusitisDiagnostic Criteria • Physical examination • Computed tomography (CT) scan
Chronic SinusitisTreatment • Pharmacologic • Glucocorticoids • Antibiotics • Nonpharmacologic • Nasal saline irrigation • Surgical
Burns • Pathophysiology • Clinical manifestations • Diagnostic criteria • Treatment
Burns Pathophysiology • Cause: direct contact with excessive heat or radiation, caustic chemicals, or electricity • Result: acute inflammatory response • Burn severity is correlated with exposure type and time
Burns Pathophysiology: Classification • Superficial partial-thickness • Deep partial-thickness • Full-thickness
Burns Clinical Manifestations • Superficial partial-thickness burns • Heat, swelling, pain, redness, loss of function • Deep partial-thickness burns • Blistering, redness, heat, pain, edema, serous exudate • Full-thickness burns • Redness, eschar, edema, exudate
Burns Diagnostic Criteria • Rule of nines
BurnsDiagnostic Criteria (cont’d) • American Burn Association has designated criteria for distinguishing minor, moderate, and major burns based on • Wound depth • Surface area • Required level of treatment
Burns Treatment • American Burn Association criteria • Remove source of injury and cool/rinse skin • Airway, breathing, circulation • Fluids, nutrition, antibiotics, analgesics • Wound management may include • Hydrotherapy • Skin grafting
Rheumatoid Arthritis (RA) • Pathophysiology • Clinical manifestations • Diagnostic criteria • Treatment
RA Pathophysiology • Chronic inflammation of synovial membranes and synovial hyperplasia • Etiology combines • Genetics • Triggering event • Autoimmunity
RA Pathophysiology (cont’d) • Remissions and exacerbations • Pannus formation • Cartilage erosion • Fibrosis • Ankylosis
RA Clinical Manifestations • Mild to debilitating • Symmetrical joints • Pain, stiffness • Redness, heat, swelling • Decreased mobility
RA Diagnostic Criteria • No definitive test • Increased likelihood with positive findings • Erythrocyte sedimentation rate (ESR) • C-reactive protein (CRP) • Rheumatoid factor (IgG) • Antinuclear antibodies (ANA)
RA Treatment • Pharmacologic: drugs that induce remission • Nonpharmacologic: • Rest/activity balance • Physical therapy exercises • Splints • Surgery
Acute and Chronic Gastritis • Pathophysiology • Clinical manifestations • Diagnostic criteria • Treatment
Acute Gastritis Pathophysiology • Ingestion of irritating substances and/or poor gastric perfusion results in acute inflammation of the gastric mucosa • Gastric epithelial cell necrosis • Gastric acid erodes underlying tissue
Acute Gastritis Clinical Manifestations • Mild to severe abdominal pain • Indigestion • Loss of appetite • Nausea • Vomiting • Hiccups
Acute Gastritis Diagnostic Criteria • History and physical examination • Endoscopic examination • Stool analysis (presence of blood in stool) • Complete blood count (anemia)
Acute Gastritis Treatment • Discontinue ingestion of irritating substance • Buffer or decrease production of gastric acid
Chronic Gastritis Pathophysiology • Chronic infection or autoimmune process leading to chronic inflammation • Infection with Helicobacter pylori bacterium • Gastric epithelial and mucosal cell atrophy • Gastric acid production impaired
Chronic Gastritis Clinical Manifestations • Dyspepsia • Loss of appetite • Vomiting • Anemia • Can be asymptomatic
Chronic Gastritis Diagnostic Criteria • Endoscopic examination • Biopsy of gastric tissue • Breath test • Blood test (protein antibodies)
Chronic Gastritis Treatment • Antibiotics for chronic infectious processes • Proton pump inhibitors or bismuth (antimicrobial and raise gastric pH) • Immunosuppressive drugs for autoimmune processes • Vitamin B12
Acute and Chronic Pancreatitis • Pathophysiology • Clinical manifestations • Diagnostic criteria • Treatment
Acute PancreatitisPathophysiology • Injury to • Acinar cells • Zymogen • Pancreatic duct • Protective digestive feedback mechanisms • Caused by • Duct blockage by gallstones • Excessive alcohol use
Acute PancreatitisPathophysiology (cont’d) • Acute pancreatitis as a result of gall stone obstruction
Acute PancreatitisClinical Manifestations • Upper abdominal pain • Sudden onset • Growing intensity • Dull, steady ache • Radiating to back • Nausea • Vomiting • Anorexia • Diarrhea
Acute PancreatitisDiagnostic Criteria • History and physical examination • Laboratory testing • Complete blood count, ESR, CRP • Serum amylase and lipase • Serum alkaline phosphatase • Total bilirubin • Aspartate aminotransferase (AST) • Alanine aminotransferase (ALT)
Acute PancreatitisTreatment • Intravenous hydration • Analgesics • Surgical removal of gallstones