Physiology sheet #2
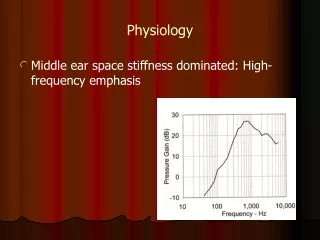
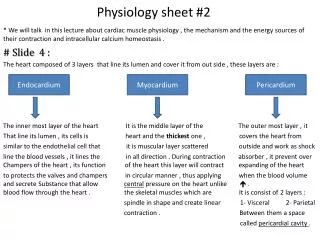
Physiology sheet #2. Endocardium. Myocardium. Pericardium. * We will talk in this lecture about cardiac muscle physiology , the mechanism and the energy sources of their contraction and intracellular calcium homeostasis . # Slide 4 :

Physiology sheet #2
E N D
Presentation Transcript
Physiology sheet #2 Endocardium Myocardium Pericardium * We will talk in this lecture about cardiac muscle physiology , the mechanism and the energy sources of their contraction and intracellular calcium homeostasis . # Slide 4 : The heart composed of 3 layers that line its lumen and cover it from out side , these layers are : The inner most layer of the heart It is the middle layer of the The outer most layer , it That line its lumen , its cells is heart and the thickest one , covers the heart from similar to the endothelial cell that it is muscular layer scattered outside and work as shock line the blood vessels , it lines the in all direction . During contraction absorber , it prevent over Champers of the heart , its function of the heart this layer will contract expanding of the heart to protects the valves and champers in circular manner , thus applying when the blood volume and secrete Substance that allow central pressure on the heart unlike . blood flow through the heart . the skeletal muscles which are It is consist of 2 layers : spindle in shape and create linear 1- Visceral 2- Parietal contraction . Between them a space called pericardial cavity .
# slide 4 continue : • The pericardial cavity is filled with fluid and proteins .In normal condition the champers will filled in normal amount but if there is infection like TB or pus in this cavity or the person had stab wound in the heart and the blood fill this space leading to accumulation of fluids or blood inside the pericardial cavity , the fluid will compress the heart preventing the normal filling of the ventricles which in turn reduce the cardiac output , this state called cardiac tamponade . • In severe condition the cardiac tamponade will reduce the cardiac output to zero , thus no blood supply to the organs and the patient will die quickly . • The patient with cardiac tamponade feels suffocating due to low blood supply that cause hypoxia , in this case the patient will taken to the hospital and the doctors will drain this fluid by a needle to relieve the symptoms by a procedure called Pericardiocentesis , if the needle was non sterilized they must remove the fluid firstly and after that give him antibiotics , they will give him fluids to compensate the lost and may given oxygen to reduce the workload of the heart as a result of decreased cardiac output . # Slide 5 : • Myocardium ==> the cells of this layer is rectangular in shape and connected to each other by gap junction through desmosomes , the gap junction is area with low resistance and it is like a gates between adjacent cells , these gates open and close according to change in the voltage , so if one cell is excited the electrical potential will pass through these junction to all cells in the heart and become excited , they depolarize at same time making contraction as one unit unlike the skeletal muscle . • The gap junction creates what we called the Syncytium , there are 2 Syncytia in the heart , atrial syncytia and ventricular syncytia . This syncytium is very important in cardiac muscle because it will make the two atriums contract together and the two ventricle contract together also , that's will enforce the blood to leave these champers in correct pathway . • The electrical impulse will pass through gap junction or ( syncytium ) and make the 2 atriums and 2 ventricles contract simultaneously at the same time as single unit .
The skeletal muscle cells is separated from each others , that means every cell must receive electrical impulse for its own , so each motor fibers in the skeletal muscle receive a branch from the motor nerve forming what we know the neuromuscular junction . # Slide 6 : • The plasma membrane in cardiac muscles called sarcolemma where as the endoplasmic reticulum called sarcoplasmic reticulum . • The sarcoplasmic reticulum in the cardiac muscle is less developed in contrast to the skeletal muscles which have well developed sarcoplasmic reticulum . The function of sarcoplasmic reticulum to store calcium ions that is needed for muscular contraction . In the skeletal muscle the stores of calcium are enough to initiate muscular contraction while in the cardiac muscle the stores of calcium aren't sufficient to create contraction but there are another source for calcium ions for cardiac muscles which is the extracellular calcium . • The sarcolemma contains invaginations called Transverse Tubules or T tubules that are wider and shorter than skeletal muscles because it contains extracellular fluid and calcium that is needed for muscular contraction compared to longer and cylindrical in skeletal muscles . • T tubules in cardiac muscle present in the Z line of sarcomere , T tubules in skeletal muscles found in I band . Each sarcomere of cardiac muscle contains only one T tubules while in skeletal muscles each sarcomere contains two T tubules . • The A and I bands are similar in cardiac and skeletal muscles , the A band is thick and I band is thin . # Slide 7 : • Gap junction is hexagonal protein structure that connect the cells together and this protein has two forms , closed and open , it opens in one direction and closed by other direction , the process of opening and closing is controlled by change in voltage , when it open the ions will flow from one cell to the other to create electrical potential and depolarize the cells to contract , gap junction forms Syncytium in cardiac muscles only not in skeletal muscles .
# Slide 8 : Because the heart is always in contractile state to pump the blood to all organs unlike the skeletal muscles that contracts when we need them to , the heart is depending on the ATP in high amounts by oxidative phosphorylation that gives large amount of ATP , so the cardiac muscles contains large numbers of mitochondria in contrast to the skeletal muscles that have few number because they derive energy from anaerobic glycolysis . The cardiac muscles have less nuclei than skeletal muscles that are rich in nuclei . # Slide 9 : we are looking to action potential in skeletal muscles : The resting membrane potential in resting cells is -70 but if the cell is stimulated by a stimulus the voltage gated channels of Na will open and Na will influx to the cell through these channel causing depolarization or raising phase until it reaches the peak where the Na channels will close, where as if the voltage gated K+ channels open the K+ will influx to the cell causing repolarization or falling phase . there are many types of channels like chemical gated channels , ligand gated channels and others. # Slide 10 – 11 : The cardiac muscle action potential Phase zero : The resting membrane potential of cardiac muscles is approximately about -80 to -90 which is more negative than skeletal muscles , as skeletal muscles when the cardiac muscles expose to certain stimulus the voltage gated Na channels will open allowing the influx of Na ions that initiatedepolarization or phase zero .
Phase 1 : The voltage gated Na channels are open and the Na enter the cell causing rapid depolarization but when these channel close and transient K channels open or influx of chloride to the cell in addition to closure of calcium channels will cause partial repolarization . • Phase 2 : The voltage gated slowca+2 ( L-type channels ) channels will open and ca+2 will influx through electrochemical gradient passively by diffusion from extracellular fluid to the cell and by closure of some K channels causing platue phase or phase 2 which the depolarization remains constant . • Phase 3 : as a result of opening in the voltage gated K channels and closure of calcium channels the repolarization will occur . • Phase 4 :The ions will rearranged in original distribution and cause resting potential where the cell become ate rest . • Note : At resting potential the conductance ( permeability ) of cell membrane to K ions is 100 higher than the Na ions because the K ions are more important in the regulation of action potential . # Slide 12 : There are 2 types of voltage gated Na channels that are embedded in the cell membrane • Extracellular gated channel called activation gate or ( m gate ) • intracellular gated channel called inactivation gate or ( h gate ) • they have the same voltage and same threshold .
At rest ( m gate ) will close and the inactivation gate ( h gate ) will open , while during depolarization the opposite will occur but the activation gates will open quickly before the inactivation gates closes allowing Na ions to influx to the cell until the inactivation gates closed , this difference in time called time constant . # Slide 13 : In phase 0 there is high permeability or conductance for Na ions to initiate action potential that might reach 500 mv per/s , while in late phase zero and early phase 1 there is decrease in k permeability and high increase in Na conductance and that's occur in cardiac muscle not in the skeletal muscles . in phase 2 the cell membrane conductance to ca+2 ions will increase while there are fast closure of K channels , the closure of K channels during phase 2 is important to maintain the platue phase. During phase 3 there is fast opening in K channels to return the cell to resting potential . # Slide 14 – 15 : check the slides for the mechanism In the cardiac muscles the calcium will come from extracellular fluid through voltage gated calcium channels and this is not found in skeletal muscles which depend only on the calcium found in sarcoplasmic reticulum . The calcium from outside will enter the cell and bind to Ryanodine receptor and cause the release of calcium of sarcoplasmic reticulum , this is called calcium induce calcium release which are found in cardiac muscles only .
# Slide 19 : Slow calcium channel blockers like verapamil and diltiazem are drugs that given to patient with cardiac failure or myocardial infarctions . The calcium concentration in extracellular fluid is much higher than its concentration intracellularly , so these drugs block these channels in the cardiac cells and reduce the ca+2 concentration inside the cell , it is working on blood vessels also to relax them and increase the blood flow and deliver the oxygen to tissues thus decrease the workload of the heart . # Slide 21 – 27 : Absolute refractory period Relative refractory period It is the period between the depolarization phase where the first stimulus stimulate the cell to the half of the partial repolarization , it is very short period and in this period no stimulus can stimulate the cell to create second depolarization even it was great stimuli because after the first action potential occurred the Na channels are inactivated ( closed ) . It is the period after the partial repolarization occurred to the end of action potential where a greater stimuli than the normal will stimulate a second depolarization .
The absolute refractory period of cardiac muscles is longer than in skeletal muscle which are very short period , the importance of this long duration in cardiac muscles because the heart is always contracting comparing with skeletal muscles that contract when we need them to , if the heart has short refractory period as skeletal muscles it will tetanize lead to death , while the skeletal muscle are exposed to tetanus when they stimulated repeatedly . • If someone have electrical shock and die , his death not because the tetanization of the heart but due to tetanization of the diaphragm which is a skeletal muscle that aids in normal respiration . The cardiac cells may tetanized due to entrapment of the Ca+2 ions inside it leading to death . • The Action potential for skeletal muscles occurs in the latent period where the muscle contracts during depolarization and relax during repolarization . • Muscle twitch which are contraction of the muscle followed by relaxation , where as in wave summation the muscle cell will expose to series of stimuli therefore unable to relax before the next stimulus is occur , so if the muscle contract due to first stimuli and couldn't relax then followed by second stimulus that create action potential stronger than the previous may lead to tetanus in the skeletal muscles if the stimulus is repeated in sufficient rate . # Slide 28 – 33 : The sarcomere which is the basic unit of a muscle consists of two proteins , myosin which forms thick filaments and actin which forms thin filaments , the actin composed of 3 types of proteins : tropomyosin : double helix strand that wrap around actin . actin : globular protein that covered by tropomyosin . Troponin : complex of regulatory protein and composed of 3 parts ( Troponin C , Troponin I , Troponin T ) . Troponin C binds calcium , Troponin I binds actin inhibitory subunit , while Troponin T binds tropomyosin .
The Mechanism of contraction • Calcium is the most important ion that connect excitation to contraction because the excitation will increase intracellular calcium that initiate muscular contraction . • the extracellular Ca+2 with Ca+2 released from sarcoplasmic reticulum bind to troponin and cause uncover of the actin binding site that binds the head of myosin . • This binding needs ATP to occur after the ATP binds it will split to ADP and inorganic phosphate , this high energy derived from the reaction will cross bridge the myosin with actin , the calcium ions will move the troponin tropomyosin complex away from the actin and myosin and leading to shortening of the sarcomere and contraction occur , the cycle repeat when new ATP is found . • Slide 42 : Frank and Starling law • << stroke volume will in response to in the volume during end of diastole (EDV) if all other factors remain constant >> . • Starling is an physiologist and in the year 1900 he called the substance secreted by endocrine glands hormones . • There is relation between the length of the muscle and its tension .
Addition notes • To calculate the ion equilibrium potential we suppose that this ion is the only ion in the cell and by applying Nernst equation to this ion we can determine its equilibrium potential , so if we need to calculate the equilibrium potential for Na ions : + 60 • that's mean the sodium ions have positive charges and will diffuse passively from higher concentration which is extracellular into the cell where they are in less concentration because Na ions have positive charges compared with the negative charges inside the cell , they create action potential . • Ca+2 has higher concentration outside the cell in contrast lower concentration inside , ca+2 ions have equilibrium potential about +125 so they will diffuse down their gradient from high outside the cell to low inside the cell , that's happen in the phase 2 or platue phase in cardiac muscles causing depolarization to make the action potential constant .