Download

1 / 57
580 likes | 603 Vues
HK Core Cardiology Certificate Course 7 April 2019 Aortic Regurgitation Dr. Yiu Siu Fung. Chronic AR. Rheumatic Connective tissue disorders / autoimmune Marfan’s syndrome Ankylosing spondylitis SLE Aortitis Syphilis. Chronic AR. Congenital Bicuspid AV VSD

E N D
HK Core Cardiology Certificate Course 7 April 2019 Aortic Regurgitation Dr. YiuSiu Fung
Chronic AR • Rheumatic • Connective tissue disorders / autoimmune • Marfan’s syndrome Ankylosing spondylitis SLE • Aortitis • Syphilis
Chronic AR • Congenital • Bicuspid AV VSD Sinus of Valsalva aneurysm • Others • HT Age related changes Myxomatous degeneration
Acute AR • Infective endocarditis • Acute aortic dissection • Congenital rupture of sinus of Valsalva • Trauma
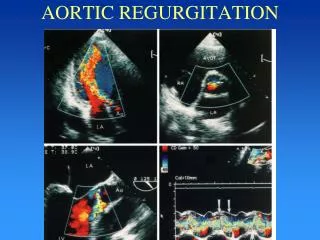
Identification of Etiology PLAX + PSAX AV morphology (cusp no, calcification, vegetations, cusp prolapse) High / R parasternal + suprasternal Thoracic aorta aneurysm + dissection +/- TEE
AV Cusp Prolapse Prolapse of non-coronary cusp AV
AV Perforation Perforation of Noncoronary Cusp due to SBE
Presentation • Chronic AR - usually no symptoms • Heart murmur • Exertional SOB, chest tightness • Heart failure • Arrhythmia
MRI / CT in AR CMR Quantify RF when echo equivocal (RV = area under aortic flow vs time curve) EF, LV volumes Aortic dilatation – max diameter FU aortic dimension (CT better than MRI – inner to inner edge technique at end diastole on strictly transverse plane by double oblique reconstruction perpendicular to axis of blood flow, NB echo: leading to leading edge)
Echo – comprehensive approach • ? Bicuspid AV • AR jet – eccentric ? (LAX), central / commisure ? (SAX) • LV size, function (small size patient – indexing LV dimension to BSA) • Aortic root / AsAo size – annulus, SOV, STJ, AsAo – leading to leading edge at end diastole, except annulus at mid systole • 3 phenotypes of AsAo (1) aortic root aneurysm SOV > 45mm (2) tubular AsAo (SOV < 40-45mm) (3) isolated AR (all diameters < 40mm) • ? AV repair / valve sparing surgery of aortic root (may need preop TEE) • Intraop TEE must if AV sparing surgery / AV repair
Functional Significance Left ventricular size and function (chronic AR) M-mode Simpson’s biplane • LVESD > 50mm • LVEF < 50%
AR Severity - Semiquantitative Methods Color Doppler • Height ratio (AR jet width / LVOT diameter in LAX) • Area ratio (AR jet area / LVOT area in SAX) Important : AR jetlengthinto LV bearsno correlation to AR severity
Color Doppler LAX / Height Ratio 2/4 AR TTE 4/4 AR TEE
Color Doppler SAX / Area Ratio 2/4 AR TTE 4/4 AR TEE
AR Severity - Semiquantitative Methods Width of Vena Contracta • Measured from PLAX view • ≥ 6mm 95% sensitive and 90% specific for diagnosing severe AR (ERO ≥ 30 mm2) • Regardless of jet direction (eccentric / central) Circulation 2000; 102: 558
AR Severity - Semiquantitative Methods PW Doppler • Descending thoracic aorta - diastolic flow reversal • Sample vol. - located near take off point of L subclavian artery AS A “QUICK AND DIRTY” METHOD, HOWEVER IS ONE OF THE MOST USEFUL SIGNS OF SIGNIFICANT REGURGITATION --- OTTO 1997
Descending Thoracic Aorta PW Doppler • Holodiastolic flow reversal – but frequent in > 60yrs subjects without severe AR (sensitivity 100% specificity 75%) • TVI > 15 cm • Peak velocity > 60 cm/s • ↑ regurgitant fraction 77% (sensitivity 100% specificity 92%) • J Heart Valve Dis. 1993 Sep;2(5):585-94 • End diastolic reversal velocity > -32.2 cm/s • J Am Soc Echocardiogr 1996;9:675-83
End-Diastolic Flow Velocity Tribouilloy C et al: Br Heart J. 1991 Jan;65(1):37-40
AR Severity - Semiquantitative Methods CW Doppler • Dense signal • PHT • If 2 separate slopes of AR velocity curve obtained - PHT should not be measured from initial steeper slope • Peak early diastolic velocity > 4m/s for accuracy • Why PHT decreases with severe AR?
CW Doppler Acute 4/4 AR due to aortic root abscess – dense signal and short PHT Chronic 2/4 AR
Pressure Curves in Chronic vs. Acute AR Solid line – chronic AR Dashed line – acute AR 100 Ao LV 0 With chronic AR, large pressure difference between LV and Ao throughout diastole With acute AR, aortic pressure falls rapidly while LVEDP elevates rapidly at end diastole → rapid equilibration of Ao and LV pressures → short PHT
AR Severity - Quantitative Methods PISA Quantitative Doppler
AR and PISA • ERO • Fundamental parameter • RV • Dependent on loading conditions • Proportional to • ERO • Pressure gradient across Ao-LV • Duration of diastole
AR and PISA AR MS
AR and PISA - Underestimation • Marked underestimation of ERO with angle of inverted aortic valvular funnel ≥ 2200 • e.g. large fusiform dilatation of Ao root • No trend of underestimation with a flat angle of flow convergence < 2200
Angle of Inverted AV Funnel ≥ 2200 Marfan syndrome with aortic root dilatation
AR and PISA • No single angle planar correction • Complex nonplanar geometry of aorta • 3D angles • Difficult on line measurement • High interobserver variability • Classification • Angle < 2200 • Angle ≥ 2200
AR and PISA • Not easy to master • High feasibility • Reliable with eccentric jet
Example of AR Quantification Grade 4/4 eccentric AR by color Doppler + high velocity holodiastolic flow reversal descending thoracic aorta (TVI = 32cm) + severe LV dilatation (49/71mm)
Continuity Equation Mitral annulus diameter 3.2cm Mitral inflow TVI 13cm LVOT diameter 2.9cm LVOT TVI 51cm
Continuity Equation • Mitral inflow stroke volume = mitral annular diameter2 x 0.785 x mitral inflow TVI = 3.22 x 0.785 x 13 = 104 cc • LVOT stroke volume = LVOT diameter2 x 0.785 x LVOT TVI = 2.92 x 0.785 x 51 = 337 cc • RV = 337 – 104 cc = 233 cc • Regurgitant fraction = RV ÷ LVOT SV = 233 ÷ 337 x 100 = 69%
PISA Apical LAX view with zoom up of AR orifice and jet Upward(not downward) baseline shift of color flow map which makes the PISA larger
PISA r = 1.31cm Vr = 52 cm/s VAR = 486cm/s TVI = 204 cm ERO = (6.28 x 1.312 x 52) ÷ 486 = 1.13 cm2 RV = ERO x AR TVI = 1.13 x 204 = 232 cc
Assessment of AR severity REMINDER All modalities have their limitations. An accurate assessment and evaluation of AR requires one to incorporate all of the available tools echocardiography provides.
Natural History of Severe AR Asymptomatic Patients + Good LV Function Excellent long term prognosis • n = 99 90% asymptomatic at 3 yrs 81% at 5 yrs 75% at 7 yrs AVR < 4% per yr Bonow et al Circulation 1983; 68: 509-517 • n = 50, EF > 50%, median FU 44 months symptomatic or LV dysfunction 4 ± 3% per yr Ann Intern Med 1989; 110:587-592
Natural History of Severe AR • n = 104, normal LV function, average FU 8 yrs Death / symptoms / LV dysfunction LVESD > 50mm19% LVESD 40-49mm 6% LVESD < 40mm 0% 2 sudden death with LVESD > 55mm Bonow et al Circulation 1991; 84:1625-35 • N = 104 FU 7.4 ± 3.7 yrs AVR / asymptomatic excessive LV ↑ / sudden death = 6.2% per yr (similar to earlier studies) Circulation 1998; 97:525-534
Natural History of Severe AR Asymptomatic Patients + Impaired LV Function 66% require surgery within 2-3 yrs Bonow et al Herz 1984; 9: 319-332 Circulation 1980; 61: 484-492 Bonow et al AJC 1982; 50: 325-336 Symptomatic Patients Poor prognosis • Only 4% alive at 10 yrs with NYHA class III or IV symptoms of CHFHenry et al Circulation 1980; 61: 484-492 • In general symptomatic CHF - dies within 2 yrs without surgery • Right sided heart failure - very poor prognosis < 10% alive at 4 yrs J Thorac Cardiovasc Surg 1981; 82: 114
Afterload Reduction in Chronic Severe AR p < 0.001 Incidence of AVR (%) Years after randomization Randomized trial of nifedipine vs. digoxin in 143 patients with chronic asymptomatic severe AR NEJM 1994; 331: 689-694
Timing of Operation in AR Previous Criteria (1) Functional Class III (2) Significant LV dysfunction Based on higher operative mortality in the past
Modern Philosophy – Earlier Surgery Based on • Enhanced understanding of natural history of AR • Lower operative risk than in the past • Newer surgical options which do not involve implantation of synthetic or non-human material
Newer Surgical Options – Role of Echo Aortic valve repair • Feasible only in 10% of AR (70% in MR) • Echo for selection • AV not thickened, retracted, calcified or restricted in motion • Diastolic leaflet prolapse of either tri- or bicuspid AV - best candidates • Aortic root dilation with otherwise normal leaflets and annulus
Aortic homograft Aortic homograft • Ideal for IE, small aortic root • Never widely used – lack of tissue donars + difficulty of OT • Echo planning OT - limited availability of valves of any given size by determining size of aortic annulus • Concerns of homograft valve failure
Indications for surgery with severe AR • Symptomatic – irrespective of LVEF
Indications for surgery with severe AR • Asymptomatic – • EF </= 50% • LVESD > 50mm • LVEDD > 70mm small body size LVESD index to BSA – 25mm/m2 • Serial rapid progression LV size or decline in EF
Indications for surgery with dilated aorta • Best defined with Marfan syndrome • Irrespective of the severity of AR