Download
1 / 14
140 likes | 276 Vues
Health among Conflict-Affected Persons in Urban Settings: key issues and documentation. Global Response 2010 Violent Conflict and Health Paul Spiegel MD, MPH Chief, Public Health and HIV Section United Nations High Commissioner for Refugees. Key Issues.

E N D
Health among Conflict-Affected Persons in Urban Settings: key issues and documentation Global Response 2010 Violent Conflict and Health Paul Spiegel MD, MPH Chief, Public Health and HIV Section United Nations High Commissioner for Refugees
Key Issues • Current strategies, policies and interventions based on older paradigms of persons of concern (PoCs)* in low income countries in camp settings • Parallel services • Dependent and confined populations (pop) • Most current conflicts are not camp settings • Urban settings or rural scattered settings • More conflicts in middle income countries * PoCs include all conflict-affected populations including refugees, internally displaced persons, asylum seekers, stateless persons, returnees, non-displaced persons, and surrounding host communities
Three-pronged Strategyto address urban health* • Advocacy • To ensure authorities make public health, nutrition, WatSan services available to these populations at low or no cost • Support • Support PoCs by integrating them into existing public services and by augmenting capacity of these systems * Designing appropriate interventions in urban settings: health, education, livelihoods, and registration for urban refugees, UNHCR, Geneva, 2009. http://www.unhcr.org/4b2789779.html
Three-pronged Strategyto address urban health (cont) 3. Assess, monitor and evaluate (M&E) to ensure adequate and equitable provision of health services • Challenging bc PoCs dispersed and may not register (e.g. protection issues) • Estimating size, demographics, and geographical distribution difficult; consequently, establishing info systems or doing pop-based surveys is complicated
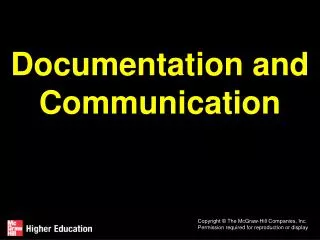
Distribution of registered Iraqi refugees and services in Damascus, Syria. UNHCR Oct 2007
Assess, M&E (cont) • Accurate pop denominator often unavailable and PoCs may use >1 health facility/provider; hence, estimating disease incidence rates and PoC usage of services is difficult • Proportional morbidity rates by facility is norm • Provides important but limited data to prioritise decision-making and to effectively M&E programmes • Sentinel sites that attempt to be representative of different parts of PoCs may be used
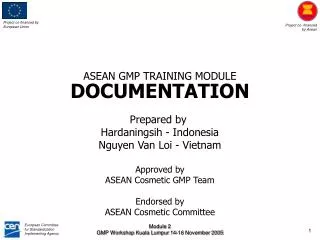
Refugee Referral Cases to Nairobi, Kenya by Disease Category: Oct 2008-Sept 2009 N=?
Assess, M&E (cont) • Integrating PoCs into existing health systems using existing health information systems (HIS) • Some HIS lack flexibility to allow for key modifications (e.g. disaggregating nationals and PoCs, adding certain disease categories) • Some HIS not provide sufficient data to allow for prioritisation of activities acc. to limited funds or to allow for effective M&E
Iraqi Refugee Patient Facility Usage and Cost, SyriaJan-Sep 2009 11
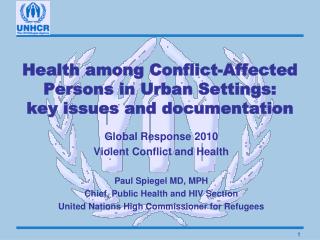
Average Cost of Referral by Disease Category, Nairobi KenyaOct 2008-Sep 2009
Assess, M&E (cont) • Pop.-based surveys proved difficult, politically controversial and bias-prone in many non-camp settings (e.g. Iraq, DRC) • Methods still require validation acc. to context • Other surveillance methods such as prospective, community-based surveillance of mortality, nut status and other key health events may be more useful in certain situations
Conclusions • Documentation of persons affected by conflict in urban settings is possible but complex • Data connection among: • Levels of care (i.e. emergency, primary, 2’ and 3’) • Patients vs. interventions • Costing • Individual and public health data needed • More expensive and sophisticated than camp settings