
Disruptive Behavior Disorders
E N D
Presentation Transcript
Disruptive Behavior Disorders MAJ Suzin Whitten, MD USAHC Baumholder, Germany 15 FEB 2007
Disruptive Behavior Disorders • What is Normal Behavior? • What Impacts the Development of Normal Behavior? • What is Temperament? • Aggression and Stress • Age Related Behavior Issues • Oppositional Defiant Disorder • Conduct Disorder • When to Refer
The Problem • Psychosocial problems in children and adolescents are on the RISE in Western cultures • Improved economic conditions and physical health
The Problem • Increasing number of office visits • Spans the biological, psychosocial, social domains • Numerous systems involved (medical, educational, legal)
What is Normal Behavior? • Society defines what is pathological • Social rules are learned • Ability to incorporate social rules developmentally over time
What is Normal Behavior? • DSM-IV-TR provides criteria to make diagnoses related to maladaptive behavior • Consider the influence of environment on behavior and behavior on environment • Understand the social context of the aggressive behavior
What Impacts the Development of Normal Behavior? • Homeostasis and adaptation • Attachment and individuation • Mastery and achievement • Environmental supports and adversities • Constitution and context
What is Temperament? • Set of individual predispositions • Underlie and modulate expression of activity, emotionality, and sociability • Reflection of baseline autonomic nervous system reactivity • Threshold, dampening, reactivation
Why Does it Matter? • Impacts development and behavior • Impacts mental and physical health • Is there a good fit?
Aggression • Stable over time and may not “grow out” • Early intervention is indicated for persistent aggressive behavior • Both genetic factors and child rearing practices contribute
Aggression • Boys > girls • Family unemployment, discord, criminality, psychiatric disorders and birth to teenage or unmarried mothers • Exposure to aggressive models on TV, in play, in life • Consider comorbid conditions
This is Your Brain on Stress • Corticotropin releasing hormone system • Locus ceruleus norepinephrine system • Limbic system
This is Your Brain on Stress Hypothalamus Limbic system CRH Emotional Pain Locus Ceruleus Pituitary Gland Vigilance Norepinephrine ACTH and B endorphins Increase BP and HR Adrenal Gland Cortisol Increased glucose metabolism
http://www.psycheducation.org/emotion/pics/big%20hypothalamus.htmhttp://www.psycheducation.org/emotion/pics/big%20hypothalamus.htm
The Link to Behavior • Reduction of autonomic responsiveness • Lower pulse rate and skin conductance in presence of arousing stimuli • Adaptive response to continual insults when exposed to stress at an early age • Lower cortisol levels, NT dysfunction
Behavior Issues: 2-4 yrs • Need for autonomy v dependence on parents, frustration and anger • Lying, impulsiveness, breath holding, defiance, and temper tantrums • Parental response is very important • 50% of preschoolers are brought to the attention of physicians for destructive and disobedient behaviors
Behavior Issues: School Age • School achievement and acceptance by peers • Lying and fantasy v lying and avoidance • Aggressive play and fighting • Stealing as impulsive, expression of anger and frustration, may be learned • Truancy, running away, and unsupervised fire starting are never developmentally appropriate
Behavior Issues: Adolescence • Progressive individuation and separation from the family • Importance of peer relationships • Intense emotions and wide swings in mood are typical • Abstraction, new mental power, omnipotence • Rigid concepts of right and wrong, idealism • Sexual activity (41% by 10th grade, 61% by 12th)
Disruptive Behavior Disorders • Oppositional Defiant Disorder • Conduct Disorder • Disruptive Behavior Disorder NOS
Assessment: History • Several sources (parent, patient, teacher) • Abuse • Trauma • Substance abuse • Specific examples of problem behaviors • Acute illness • Chronicity
Assessment: Physical • Complete neurological exam and detailed age appropriate mental status exam • No specific laboratory tests or radiological studies • Consider psychological testing
“He’s ODD?” • 9 y/o male with Type I DM and ADHD going “nuts” in the clinic • “Uncontrollable” • Wielded knife in kitchen, tried to hit Mom • Cursing and yelling • Not going to school and failing all classes • Father is deployed
Oppositional Defiant Disorder A pattern of negativistic, hostile, and defiant behavior lasting at least 6 mos, during which 4 or more of the following are present: 1) often loses temper 2) often argues with adults 3) often actively defies or refuses to comply with adults’ requests or rules 4) often deliberately annoys people 5) often blames others for his/her mistakes 6) often touchy or easily annoyed by others 7) often angry or resentful 8) often spiteful or vindictive DSM IV TR, 2000
Oppositional Defiant Disorder • 2 to 16 % • Boys before puberty, equal after puberty • NET age 3, evident before age 8, NLT than 11 • Gradual onset, emerge in home setting • May be the antecedent to Conduct Disorder but usually does not persist after adolescence
ODD: DDx • Conduct Disorder • Mood Disorder • Psychotic Disorder • ADHD (may be co-occur) • Mental Retardation • Learning Disorder • Normal individuation of adolescence
Treatment: ODD • Parent training to manage child behavior • Child individual therapy to develop efficient anger management, decrease negativity, and improve social skills • Family therapy to improve communication
Parent Behavior from AACAP • Build on positives, give praise and reinforcement when child shows flexibility and cooperation • Demo desired role model behavior by taking a time out when upset • Pick battles and set priorities for what they want to do to minimize power struggles
Parent Behavior from AACAP • Establish reasonable, age appropriate limits with consequences that are consistently enforced • Maintain other interests • Work with and obtain support from other adults who interact with child • Manage own stress and use respite care when needed
Conduct Disorder A repetitive and persistent pattern of behavior in which the basic rights of others or major age appropriate societal norms or rules are violated, as manifested by the presence of 3 or more of the following criteria for the past 12 mos with one criterion present in the past 6 mos: DSM IV TR, 2000
Conduct Disorder • 15 criterion that are broken down into 4 categories 1) Aggression to people and animals 2) Destruction of Property 3) Deceitfulness or Theft 4) Serious Violation of Rules DSM IV TR, 2000
Conduct Disorder: Childhood Onset • Age < 10 • Male > female • Frequently display physical aggression • Have disturbed peer relationships • ODD during early childhood • Concurrent ADHD is common • Greater risk for Antisocial Personality D/O
Conduct Disorder: Adolescent Type • Age > 10 • Less likely to display physical aggression • More normative peer relationships • Less likely to persist beyond adolescence • Less likely to develop ASPD
Conduct Disorder • More common in urban settings • 6-16% males, 2 to 9 % females • More likely to die from homicide, suicide, violent accident, drug overdose • Associated with lower than average intelligence, particularly verbal IQ
Conduct Disorder: Comorbid • ADHD is common (30 - 50%) • Learning disorders (10 – 90%) • Anxiety d/o (15 - 24%) • Depressive d/o (15 - 24%) • Substance Related d/o (? >80%) • 25 to 40% of kids with CD go on to develop ASPD
ODD ADHD Mood d/o (Bipolar) Adjustment d/o Child or Adolescent Antisocial Behavior Mental Retardation Psychotic d/o Head Trauma Seizure Disorder Birth Injury to the Brain Encephalitis Conduct Disorder: DDx
Conduct Disorder: Risk Factors • Parental rejection and neglect • Difficult infant temperament • Inconsistent child rearing practices with harsh discipline • Physical or sexual abuse
Conduct Disorder: Risk Factors • Lack of supervision • Early institutional living • Frequent change of caregiver • Large family size • History of maternal smoking during pregnancy
Conduct Disorder: Risk Factors • Peer rejection • Association with delinquent peer group • Neighborhood exposure to violence • Familial psychopathology (ASPD, substance dependence)
Treatment: CD • Parent management training • Social Cognitive and problem solving skills training • Peer and school based interventions • Community intervention strategies
Treatment: CD • Treatment of comorbid disorders • Individual, psychodynamic therapy not effective • Early intervention > later intervention
“Is he ODD?” • 9 y/o male with Type I DM and ADHD going “nuts” in the clinic • “Uncontrollable” • Wielded knife in kitchen, hit Mom • Cursing and yelling • Not going to school and failing all classes • Father is deployed
Role of Pharmacotherapy • Not yet clearly defined • Referral to initiate pharmacotherapy • Treatment of concurrent disorders
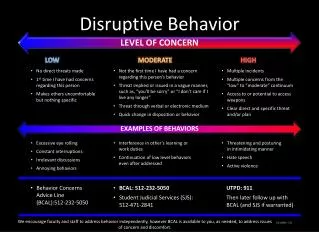
When to Refer • Harm to self or others • Rapidly escalating in severity • Ineffective interventions • Multiple domains of pathology
A few words parting words about ADHD • Most commonly diagnosed behavioral disorder of childhood • Inattention persists • Consider COMORBID conditions!!! • 33% with ODD, 35% with CD, <20% with depressive d/o, 25% anxiety d/o, 12% learning d/o
Resources for Parent/Clinician • Taking Charge of ADHD: The Complete, Authoritative Guide for Parents by Russell A. Barkley • Your Defiant Child: Eight Steps to Better Behavior by Russell A. Barkley • 1-2-3 Magic: Effective Discipline for Children 2-12 by Thomas W. Phelan • Your Adolescent by AACAP edited by Dr. David B. Pruitt • Your Child by AACAP edited by Dr. David B. Pruitt • The Explosive Child by Ross W. Greene, Ph.D. • Defiant Children, 2nd Ed: A Clinician’s Manual for Assessment and Parent Training by Russell A. Barkley • Attention-Deficit Hyperactivity Disorder, 3rd Ed: A Clinical Workbook by Russell A. Barkley and Kevin R. Murphy