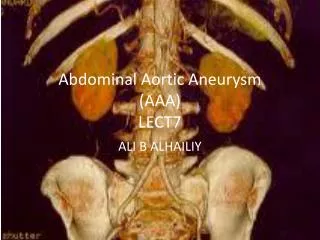
Abdominal aortic disease
עדי ר. בכר כלי דם שערי-צדק. Abdominal aortic disease. Aneurysms are focal dilatations of a 50% larger than the expected normal arterial diameter. Normal aortic diameter is 1-2 cm. Typically diagnosed if aortic diameter is ≥ 3.0 cm

Abdominal aortic disease
E N D
Presentation Transcript
עדי ר. בכר כלי דם שערי-צדק Abdominal aortic disease
Aneurysms are focal dilatations of a 50% larger than the expected normal arterial diameter. Normal aortic diameter is 1-2 cm. Typically diagnosed if aortic diameter is ≥ 3.0 cm Nearly all AAAs involve the infrarenal aorta, 25% of AAAs also involve the iliac arteries. background
In the US, AAA causes almost 14 000 deaths each year and accounts for 63 000 hospital discharges Prevalence of AAA
Abdominal aortic aneurysm (AAA) is diagnosed in 5%–10% of men above the age of 65. • There is mounting evidence that the population aged above 80 years will significantly increase over the next 20 years.
Multivariabie Models of Factors Associated with Abdominal Aortic Aneurysm as Defined by Infrarenal Aortic Diameter Aortic Diameter 3,0-3,9 cm Compared vi/ith < 3.0 cm Aortic Diameter -- 4,0 cm Compared with < 3 0 cm 1.52(1.45-1,60) 0,62(0,41-0.94) 0.72 (0.59-0.87) 0,85(0,67-1.09) 1.20(1.14-1.26) 0 97(0,89-1,06) 1 06(0,98-1,14) 1.96(1,68-2,28) 2. 72(2,37-3,11) 1.25(1,14-1,37) 1,33(1,20-1,48) 1.42(1,30-1,55) 1.39(1 20-1,62) 1-22(1,09-1,37) 0 90(0 76-1,06) 0.68(0,60-0 77) 1.04(0,92-1 16) 0.90(0,80-1,03) 1.06(0,96-1,18) Age (per 7-year intervaD^: Female se;< Black race (compared with white) Other race (compared with white) Height (per 7-cm intervai)* Weight (per 16-kg interval)-t Waist circumference (per 11 -cm tnterval)1 Family history of abdominal aortic aneurysm History of smoking§ Hypertension High cholesterol levels Coronary artery disease Claudication Cerebral vascular disease Deep venous thrombosis Diabetes mellitus Chronic obstructive pulmonary disease Cancer at site other than skin Abdominal imaging in past 5 years • 1.65(1,53-1.78) • 0.22(0,07-0,68) • 0 49(0,35-0,69) • 0 91 (0,63-1,33) • 1,21 (1,12-1 30) • 1.08(0,95 1 23) • 1.15(1,03-1,29) • 1.95(1 56-2 43) • 5.57(4,24-7,31) • 1,16(1,01-1,32) • 1,54(1,31-1.80) • 1-62(1,41-1.84) • 0,96(0,74-1,25) • 1 19(0,99-1.42) • 0,67(0.50-0.881 • 0,54(0,44-0.65) • 1-28(1,09-1,50) • 0,90(0,74-1,09) • 0,80(0,67-0,94) March 1997 • Annals of Intenud Medicine • Volume 126 • Number 6
Prevalence of Abdominal Aortic Aneurysm 4.0 cm or Larger Detected by Screening in Men 15 March 1997 • Annals of Internal Medicine • Volume I2. Number 6
Destruction of the structural and cellular components of the aortic wall Proteolitic degradation of the elstin lead to weakening dilatation. Progressive irreversible degeneration of the elastic media Etiology and Pathogenesis of AAA
Degradation in the aneurysm wall is contributed by the matrix metalloproteinase family (MMP) Several studies suggested an imbalance between MMP and TIMPs (tissue inhibitor of metalloproteinase)
Pathogenesis of AAA Circulation Journal Vol.77, December 2013
A promising potential molecular target of pharmacological treatment for AAA is MMPs Other potential medical treatments include anti-hypertensives, statins, and antibiotics. (some of which might work as MMP inhibitors) Medical Treatments for AAA
Hypothesis: Propranolol might affect the growth of an aneurysm by lowering blood pressure and its biochemical effects on matrix proteins. Several animal studies have indicated that propranolol reduces the growth of an aneurysm and rupture risk. Propranolol for small abdominal aortic aneurysms: results of a randomized trial.(JVS 2002 Jan;35(1):72-9) Patients with AAAs do not tolerate propranolol well, and the drug did not significantly affect the growth rate of small AAAs Beta-Blockers
ACE inhibitors have found to both stimulate and inhibit MMPs depending on cell types and animal models Transforming growth factor-β (TGF-β) plays an important role in the pathogenesis of Marfan syndrome- Losartan, an ARB and also TGF-β antagonism suppressed the progressive matrix degradation in the mouse model of Marfan syndrome. Results are inconsistent yet Angiotensin-Converting Enzyme Inhibitors (ACE Inhibitors)and Angiotensin Receptor Blockers (ARB)
It has pleiotropic effects such as anti-inflammatory activities and has the ability to stabilize plaque as well as to control serum lipid levels. Although statins are expected to be one of the promising drugs for the medical treatment of AAA, further studies are still needed to establish the evidence of their beneficial effects Statin
Several studies have reported that Chlamydia pneumoniae(C. pneumoniae) has been associated with the atherosclerotic lesions of arteries. Few discrepant studies that do not clarify the pharmacological mechanism in respect to the development of AAA, and no clear beneficial effect on AAA expansion Macrolides
There are numerous reports with respect to the suppressive effects on MMP by tetracycline. There is some limited evidence that Doxycylin may have a slight protective effect in retarding the expansion rates of small AAAs. Further investigation is required. Tetracycline (Doxycycline)
SVS Guideline Recommendation in the Medical Management of AAA During the Surveillance Period Quality of Evidence Level of Recommendation
Risk of rupture for untreated aneurysm within 5 years (%) AAA: risk of rupture 75% 80 70 60 50 35% 40 25% 30 20 10 0 5-5.9cm 6-6.9cm ≥7cm Aneurysm size
Ruptured AAA Mortality rate can be as high as 80% More than one third of rupture cases die outside the hospital Rupture outcomes
ACC/AHA Guidelines AAA repair Infrarenal AAA ≥ 5.5 cm should undergo repair Infrarenal AAA size 4.0-5.4 cm, ultrasound/CT scans every 6-12 mo AAA <4.0cm, ultrasound every 1-2 years is reasonable Intervention not recommended asymptomatic infrarenal/ juxtarenal AAAs <5.0 cm (men) or <4.5 cm (women)
Female gender Rapid expansion- aneurysm growth of >5 mm in six months or 10 mm per year Coexistent aneurysm or PAD Symptomatic patient Other considerations
Abdominal/back/flank pain — Patients presenting with abdominal/back/flank pain in association with AAA should be admitted for further evaluation and monitoring Thromboembolism Aortic infection Inflammatory aneurysm Symptomatic AAA
Treatment options Endovascular stent grafting • Open surgery
Established procedure more than 40 years of clinical experience Excludes aneurysm and prevents sac growth Proven, long-term results Open repair: advantages
Open repair: Disadvantages • Significant incision in the abdomen • 30–90 minute cross-clamp • Up to 4-hour procedure • 1–2 days intensive care7–14 days hospitalization4–6 weeks recovery time
Patients Don’t Want a Big Operation Prolonged convalescence Complications
Endovascular aneurysm repair (EVAR) • Benefits • minimally invasive • reduced risk of perioperative death • faster recovery
Arteriotomy devise insertion
Fluoroscopy of Talent StentgraftInside deliverysystem catheter Flexible tip Sheath marker FreeFlo Distal radio-opaques markers
Final Angiogram • Complete lining of the arterial wall, exclusion of the aneurysm sac with no residual blood flow (endoleak)
Anatomic suitability Aortic neck diameter Aortic neck length Aortic neck angulation Iliac artery and access vessel morphology
Postprocedural Renal Impairment observed a 10% decrease in creatinine clearance over the first year Life table analysis suggests that between 25% and 36% of EVAR patients have developed renal impairment by 3 years after the procedure, which compares to a 19% rate of renal impairment at 3 years following open repair. EVAR produces a steady deterioration in renal function over time Long term comlication
Device migration after endovascular aneurysm repair