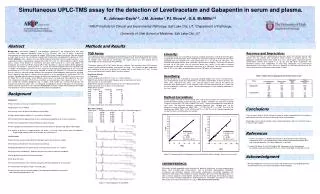
Download

1 / 35
360 likes | 585 Vues
Adjunctive Therapy for PCI. Neal Uren MD MRCP Department of Cardiology Royal Infirmary of Edinburgh. Determinants of Successful PCI. CLINICAL STATUS LV function Stable vs. unstable angina vs. MI LESION COMPLEXITY AHA/ACC class OPERATOR VOLUME ADJUNCTIVE THERAPY

E N D
Adjunctive Therapy for PCI Neal Uren MD MRCP Department of Cardiology Royal Infirmary of Edinburgh
Determinants of Successful PCI CLINICAL STATUS • LV function • Stable vs. unstable angina vs. MI LESION COMPLEXITY • AHA/ACC class OPERATOR VOLUME ADJUNCTIVE THERAPY • Stenting (BENESTENT, STRESS) • Anti-thrombotic and anti-platelet agents
Rationale “Although it is not yet possible to pharmacologically modify the risk of balloon-mediated intimal and medial disruption, it is possible to modify chemically the platelet-fibrin response to vascular injury in order to influence the outcome of the procedure”
Pharmacological Adjunctive Therapy • Heparin • Aspirin • Clopidogrel • Glycoprotein IIb/IIIa inhibitors
UK Interventional Practice 1999 • Structured questionnaire • 68% response over 4 months • 53% ≥10,000 U heparin • 8.3% abciximab use • 82% clopidogrel use Swanson N et al, Int J Cardiol 2001;79:119-125
Heparin • Lower incidence of complications in unstable angina patients pre-treated with iv heparin Lukas MA et al, JACC 1988;11:132A(abstr) • Close temporal relationship between discontinuation of anticoagulation after PTCA and coronary occlusion Gabliani G et al, AHJ 1988;116:696-700 • 10,000 U iv heparin = ACT <300s in 5% of stable and 15% of unstable patients Dougherty KG et al, CCD 1992;26:260-3
Defining the Optimal ACT with UF Heparin • Meta-analysis of 6 trials with UFH as control • n=5216, with patients in 25 s intervals • Endpoint of 7 day MACE + major/minor bleeds • ACT 350-375 s 6.6% vs ACT 171-295 s 8.8% (p<0.01) • ACT should be substantially higher than currently appreciated Chew DP et al, Circulation 2001;103:961-6
Low Dose Heparin (30 U/kg) • n=418 patients • Mean age 63±11 years • 2253±1056 U/l with a final ACT of 174±69 s • Manual compression for 7.7±3 minutes • Average procedure time of 25±16 minutes • MACE 2.9% at discharge • 0.24% serious vascular complications Godon P et al, Arch Mal Coeur Vaiss 2001;94:984-8
Low Molecular Weight Heparin • Elective PCI • NICE 1 = enoxaparin 1.0 mg/kg iv • NICE 4 = enoxaparin 0.75 mg/kg iv with standard abciximab • Comparable incidence of bleeding and ischaemic complications in NICE 4 compared with UFH + abciximab Kereiakes DJ et al, J Invas Cardiol 2001;13:272-8
Low Molecular Weight Heparin 2 doses of Dalteparin + abciximab (n=57) 12 10 8 40 U/kg 6 60 U/kg 4 2 0 Procedural thrombosis Major bleeding Kereiakes DJ et al, Am Heart J 2001;141:348-52
Aspirin • No difference in outcome between 80 mg and 1500 mg started 24 h pre-PCI Mufson L et al, JACC 1988;11:236A(abstr) • No additional benefit of dipyridamole Lembo NJ et al, AJC 1990;65:422-6 • No benefit from single dose ASA pre-PCI Patrono C et al, Circulation 1985;72:1177-84
Ticlopidine Study Trial Ischaemic complications after 4-5 days pre-treatment Placebo 14 ASA 325mg2 +Persantin 75 mg3 12 Ticlopidine 250 mg3 10 8 Percentage 6 4 2 0 White CW et al, Circulation 1987;76:IV-400
Platelet Aggregability Post-PCI * p=0.06 p=0.06 120 p=0.03 * Greater aggregability 100 * 80 Time to occlusion (s) 60 40 ASA+Ticlid PTCA 20 ASA Coronary angio 0 Pre Post Fischetti D et al, J Thromb Thrombolysis 2001;10:265-9
De-evolution of Stent Thrombosis 1986-91 Serruys et al/Schatz et al ~25% 1991 10 pooled studies 4.5% 1993 Stress/Benestent/TASC 1 3.7% 1994 Colombo et al 0.9% 1995 MUST Registry 1.6% 1996 MUSIC Registry 0.6% 1997 Moussa et al 1.9%
Risk of MACE After Successful Stenting • Age • n=2894 105 events • Diabetes • • • Acute MI (<72h) • Unstable angina • Impaired LV • • Stented length • • Residual dissection • • • Stent overlap • • • Use of ticlopidine* 0.1 1.0 10 20 0.1 1.0 10 20 Hazard Ratio & 95% CI Hazard Ratio & 95% CI * 80% ASA+Ticlidopine Schülen et al, Circulation 1998;98:104-111
Risk of a Procedural Failure Procedure failure = MACE 42.6%, procedure success = MACE 3.6% CFX or SVG • • Vessel size • • Stenosis grade • • Stenosis length • • Acute occlusion pre-stent • • Experience (yrs) • • 0.1 1.0 10 20 0.1 1.0 10 20 Odds Ratio & 95% CI Odds Ratio & 95% CI Schülen et al, Circulation 1998;98:104-111
The STARS Trial 1965 patients 50 centres 84% angio. success 7 6 5 Percentage 4 Aspirin 3 Aspirin+Warfarin * Aspirin +Ticlopidine 2 * 1 0 Stent Thrombosis at 30 days Haemorrhagic * p<0.001 vs. others complications Leon MB et al, NEJM 1998;339:1702-4
The STARS Trial Suboptimal Stent Registry 265 patients 16% vs.27% 9/12 CRS * 9 8 7 Multiple stents Low final MLD No ticlopidine 6 5 Percentage * 4 Optimal (<10%DS) 3 Suboptimal * 2 1 0 30 day stent thrombosis 30 day Peri- * p<0.01 mortality procedure NQWMI Cutlip DE et al, JACC 1999;34:698-706
Clopidogrel vs. Ticlopidine Post-PCI • No one trial large enough to demonstrate comparability • n=13,995 meta-analysis • 1° endpoint of MACE at 30 days after stenting • MACE clopidogrel = 2.1% vs MACE ticlopidine = 4.0% • Death clopidogrel = 0.48% vs death ticlopidine = 1.1% • Bhatt Dl et al, JACC 2002;39:9-14
MACE Post-Stenting Bhatt Dl et al, JACC 2002;39:9-14
30 Day Mortality Post-Stenting Bhatt Dl et al, JACC 2002;39:9-14
Duration of Therapy • Retrospective analysis of ticlopidine post-stent • n=5678 • 2.0% stent failure at 2 weeks + 0.5% at 2-4 weeks • Risk factors for late events (2.5% if all 3 present) - age - reduced LV function - hypertension • 4 weeks theinopyridine therapy preferable Schülen H et al, JACC 37:2066-73
Timing of Therapy • Ticlopidine >24 h pre-PCI cause significant platelet inhibition • Maximum effect at 3-5 days van de Loo A et al, Eur Heart J 1998;19:96-102 • Ticlopidine pre-treatment duration ~ reduced NQWMI Steinbuhl S et al, JACc 1998;32:1366-70 • Clopidogrel induces platelet inhibition within 30 min • MACE ~ no pre-treatment (T / C) [OR 3.5] Steven P et al, JACC 2001;38:648A (abstr)
Placebo Reopro B+I Glycoprotein IIb/IIIa Receptor Inhibition30 day MACE with Abciximab EPICEPILOGCAPTURE High-risk PCIRefractory USA pre-PCI 14 20 12.8% 12 35% 11.7% 29% 15 15.9% 10 8 Percentage 8.3% 55% 10 11.3% 6 5.3% 4 5 2 0 0 n=2099 n=2972 n=1265 NEJM1994;330:957 NEJM 1997;336:1689 Lancet 1997;349:1429
EPILOG & Bleeding Risk Low dose heparin = 70 U/kg for ACT≥200 s Stnadard dose heparin = 100 U/kg for ACT≥300 s
MACE in the CAPTURE trial by TnT Hamm CW et al, NEJM 1999;340:1623
The EPISTENT Trial • 63 centres in North America • 2399 patients undergoing PCI • 36% unstable angina <48h • 57% unstable angina <6 months • 16% recent MI (<7 days) • 20% diabetics • Reopro 60 min pre-PCI, 12 h post-PCI Lancet 1998;352:87
EPISTENT at 30 Days and 12 Months Death/MI/Urgent Revascularisation * 20 Stent + placebo 15 51% 52% Stent + abciximab % Balloon + abciximab 10 ° * * * * p<0.01, ° p<0.05 5 0 30 day MACE Death/MI TVR 1 year Lancet 1998;352:87
EPISTENT Subgroup Analysis Lancet 1998;352:87
EPISTENT Subgroup Analysis Reduction of Non-Q wave MI Lancet 1998;352:87
Conclusions • Heparin - lower doses acceptable (?<5000 U) • Pre-treatment with aspirin essential • Clopidogrel pre- & post-stenting • GpIIb/IIIa receptor inhibitors - Reopro™ reduces CK release in stable angina • No substitute for optimal stent deployment