BASIC SCIENCE: ATHEROSCLEROSIS
BASIC SCIENCE: ATHEROSCLEROSIS. 2 February 2006 St Luke’s-Roosevelt Hospital Department of Surgery. Which of the following are risk factors for atherosclerosis? Hypercholesterolemia Hypertension High HDL levels Cigarette smoking Diabetes Hypohomocysteinemia.

BASIC SCIENCE: ATHEROSCLEROSIS
E N D
Presentation Transcript
BASIC SCIENCE: ATHEROSCLEROSIS 2 February 2006 St Luke’s-Roosevelt Hospital Department of Surgery
Which of the following are risk factors for atherosclerosis? • Hypercholesterolemia • Hypertension • High HDL levels • Cigarette smoking • Diabetes • Hypohomocysteinemia
Which of the following are risk factors for atherosclerosis? • Hypercholesterolemia • Hypertension • High HDL levels • Cigarette smoking • Diabetes • Hypohomocysteinemia
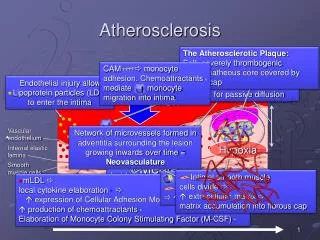
Which of the following is/are true about the pathogenesis of atherosclerosis? • Atheromas are thought to be the result of endothelial response to injury. • Atherosclerotic plaques tend to form at vascular bifurcations. • Atherosclerotic plaques progress with time. • The vascular smooth muscle cell changes from a secretory to contractile state during atherogenesis. • PDGF (platelet derived growth factor) is a potent stimulator for migration and proliferation of macrophages.
Which of the following is/are true about the pathogenesis of atherosclerosis? • Atheromas are thought to be the result of endothelial response to injury. • Atherosclerotic plaques tend to form at vascular bifurcations. • Atherosclerotic plaques progress with time. (FALSE, may regress, progress, or stay stable with time) D. The vascular smooth muscle cell changes from a secretory to contractile state during atherogenesis. (FALSE, changes from contractile to secretory.) E. PDGF (platelet derived growth factor) is a potent stimulator for migration and proliferation of macrophages. (FALSE, stimulator of vascular smooth muscle cells.)
Preservation of arterial luminal area occurs by enlargement of the arterial wall until what amount of plaque volume (beyond which compensation fails and the lumen progressively narrows with plaque enlargement)? • 20% • 40% • 60% • 80% • 90%
Preservation of arterial luminal area occurs by enlargement of the arterial wall until what amount of plaque volume (beyond which compensation fails and the lumen progressively narrows with plaque enlargement)? • 20% • 40% • 60% • 80% • 90%
Buerger’s disease Takayasu’s arteritis Temporal arteritis Raynaud’s phenomenon Involves aorta and major branches, may present as arm claudication Involves superficial temporal art., vertebral art., and aorta, may present with facial muscle claudication Associated with smoking, arterial involvement progresses from distal to proximal Associated with cold exposure or stress, recurrent episodic vasoconstriction of digits Match the following
Buerger’s disease Takayasu’s arteritis Temporal arteritis Raynaud’s phenomenon Involves aorta and major branches, may present as arm claudication Involves superficial temporal art., vertebral art., and aorta, may present with facial muscle claudication Associated with smoking, arterial involvement progresses from distal to proximal Associated with cold exposure or stress, recurrent episodic vasoconstriction of digits Match the following
Define ABI testing. What are the accepted values for claudication and rest pain?
Define ABI testing. Ankle-brachial index: DP/PT systolic blood pressure/brachial systolic blood pressure What are the accepted values for claudication and rest pain? Normal 1.0 – 1.2 Claudication 0.5 - 0.7 Rest pain < 0.4 (reflects critical ischemia)
Why might ABI measurements be inaccurate in diabetic patients? What further provocative testing can be done if a patient complains of claudication but has a normal ABI value?
Why might ABI measurements be inaccurate in diabetic patients? Vessel calcification may cause the vessels to be difficult to compress, increasing ankle BP resulting in falsely elevated ABI. What further provocative testing can be done if a patient complains of claudication but has a normal ABI value? ABI post-exercise
Describe the location of the lesion seen on the PVRs. Occlusive disease on the right aortoiliac and popliteal region.
Doppler ultrasound can be used in surveillance of post-op grafts. Which of the following is consistent with critical hemodynamic lesion? • Peak systolic velocity > 300cm/sec, velocity ratio (lesion/upstream) > 3.5, and overall graft velocity < 40cm/sec • Peak systolic velocity < 150cm/sec, velocity ratio (lesion/upstream) < 1.5, and overall graft velocity < 40cm/sec • Peak systolic velocity > 300cm/sec, velocity ratio (lesion/upstream) > 3.5, and overall graft velocity > 80cm/sec • Peak systolic velocity < 150cm/sec, velocity ratio (lesion/upstream) < 1.5, and overall graft velocity > 80cm/sec • Peak systolic velocity < 150cm/sec, velocity ratio (lesion/upstream) > 3.5, and overall graft velocity < 40cm/sec
Doppler ultrasound can be used in surveillance of post-op grafts. Which of the following is consistent with critical hemodynamic lesion? • Peak systolic velocity > 300cm/sec, velocity ratio (lesion/upstream) > 3.5, and overall graft velocity < 40cm/sec • Peak systolic velocity < 150cm/sec, velocity ratio (lesion/upstream) < 1.5, and overall graft velocity < 40cm/sec • Peak systolic velocity > 300cm/sec, velocity ratio (lesion/upstream) > 3.5, and overall graft velocity > 80cm/sec • Peak systolic velocity < 150cm/sec, velocity ratio (lesion/upstream) < 1.5, and overall graft velocity > 80cm/sec • Peak systolic velocity < 150cm/sec, velocity ratio (lesion/upstream) > 3.5, and overall graft velocity < 40cm/sec
Which of the following is/are true about transcutaneous oximetry? • Variables such as skin temperature, sympathetic tone, and skin conditions may effect this test. • Values greater then 10mmHg are predictive of healing of foot lesions. • Useful for the evaluation of diabetics with extensive calcification to determine critical ischemia. • Measures oxygen tension in the skin to assess tissue perfusion.
Which of the following is/are true about transcutaneous oximetry? • Variables such as skin temperature, sympathetic tone, and skin conditions may effect this test. • Values greater then 10mmHg are predictive of healing of foot lesions. (FALSE, greater then 40mmHg, less then 10mmHg consistent with critical ischemia.) C. Useful for the evaluation of diabetics with extensive calcification to determine critical ischemia. D. Measures oxygen tension in the skin to assess tissue perfusion.
List some potential complications of angiography as related to catheterization and the injected contrast dye.
Puncture Site Related Hematoma Hemorrhage Pseudoaneurysm AV fistula Atheroembolization Local thrombosis Contrast Related Anaphylaxis Sensitivity reactions Vasodilation / hypotension Nephrotoxicity Hypervolemia List some potential complications of angiography as related to catheterization and the injected contrast dye.
What is the most important measure to protect the kidneys from contrast induced nephropathy?
What is the most important measure to protect the kidneys from contrast induced nephropathy? Maintain adequate hydration—before, during, and after the angiography is done.