Download
1 / 12
120 likes | 484 Vues
This informative pack provides guidelines for pressure ulcer prevention in both community and inpatient settings. It includes risk assessment tools, skin inspection recommendations, and strategies to minimize risks through comprehensive care planning. The pack emphasizes the importance of regular assessments, consent for skin inspections, and prompt actions upon identifying skin changes. Nurses are guided on utilizing Walsall and Waterlow scores, addressing specific risk factors, and integrating patient education into care plans. The pack also covers equipment usage and the importance of timely assessments to prevent pressure ulcers effectively.

E N D
Pressure Ulcer Prevention Information Pack for Bank & Agency Nurses
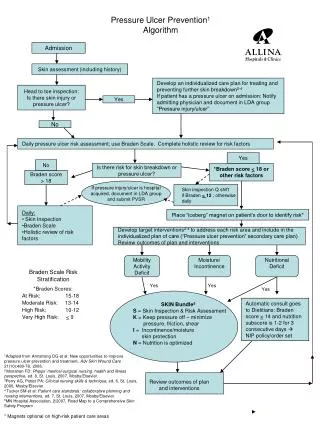
R isk Assessment Assess Assess on first contact (Community) & within 6 hours of admission (Inpatients) Walsall Score for Community & Waterlow for Inpatients Re-assessment guide (minimum requirement – may need to be more frequent in accordance with the patient’s clinical condition): Advice Use the “Tell Us” leaflet to encourage patients to engage & report if they are at risk from changes to their condition/circumstances Action Walsall / Waterlow risk assessments must be used alongside clinical judgement, skin assessment and consideration of support surfaces. Make links between the assessments and utilise clinical judgment Review assessments will include a repeat of the screening tool, a visual or verbal skin inspection, a check of the equipment and a review of the plan of care. Address each risk factor in your plan of care to minimise the risks. A separate care plan needs to be developed to target specific risks, e.g. moisture lesions, heavy oedematous limbs & subsequent reduction of pressure to the patient’s heels, reduced sensation & triggers for regular repositioning If the patient has had a previous pressure ulcer, they are immediately at risk of developing another, regardless of the current risk assessment.
Assess Gain consent from the patient to inspect their skin Complete a comprehensive skin inspection on admission, discharge/transfer & at regular intervals depending on the outcome of the initial skin inspection, risk assessments & subsequent changes to the patient’s condition. For inpatients this may be daily if at risk of pressure damage to TDS if high at risk. In the community this will be 3 monthly if at risk, 2 monthly if medium-high risk & monthly if high – very high at risk. Undertake a top – toe skin inspection, paying particular attention to bony prominences Inspect the skin at every clinical opportunity Increase this frequency of there are any signs of redness &/or pressure damage: & act on this Look for: Unresolving redness or non-blanching redness over bony prominences (normal redness from pressure should resolve within half an hour) Feel for:Altered skin texture/tone over bony prominences – softness, spongey, induration (hardness), boggy. Altered skin temperature between bony prominence & adjacent skin (hot/cold) Listen for: Patient reports of pain, numbness, burning, soreness or itching over bony prominences The look – listen – feel approach is especially importance with patients with darker pigmented skin where redness may not be present Use a mirror to inspect awkward areas such as under heels Remove dressings if you do not know what this skin is like underneath. If there are no contra-indications, remove any splints to check the skin Verbal response for an assessment may be ok for one assessment but visual is advised for the next skin inspection
Advice Explain to the patient/carer the reason for skin inspections & ensure they understand Encourage patients / their carers to inspect skin. Provide advice on what to look for & give the Patient Information booklet on Prevention of Pressure Ulcers & “Tell Us” leaflet. If the patient does not speak English provide them with the “Talking Leaflet” Ask patients, carers and families to complete the Think SSKIN chart whenever the opportunity arises. If the patient declines a skin inspection, ascertain the reason for this & document. Can this be overcome in anyway? Complete the Decisions against Advice Form if this becomes recurrent & cannot be resolved Action Complete a skin inspection chart. Once redness or skin changes are occurring, change the plan of care immediately & address any pressure to minimise the risk of further damage. Document any other skin issues on the body map or wound assessment chart as appropriate See separate pressure ulcer grading & moisture lesion recognition charts in pack for guidance on how to assess severity/identify Gain consent & photograph pressure ulcers Relay any findings (including all grades of PU) & actions to the Team Leader/Nurse in Charge asap
Assess Ensure a timely assessment for equipment takes place – do not wait for the risk assessment to be completed Anyone with a pressure ulcer should have a mattress replacement system or targeted pressure relief on admission. Any patient that sits out for longer than 2 hours requires a pressure reducing cushion as well as repositioning. Use the equipment flow chart to help in determining appropriate equipment Advice Discuss equipment with patients, relatives & carers. Show them how to use it & check it. Document you have undertaken this. Check they understand & re-check at subsequent visits Action Anyone immobile requires equipment to assist in the prevention of pressure ulcers. Think Heels - utilise targeted pressure relieving equipment such as Repose Foot Protectors, Heel Lift Suspension Boots or Dermal Pads. Link any changes to skin inspection and step up equipment. Address all surfaces: Bed: consider a foam, Repose or alternating air mattress. Chair: utilise a foam or Repose cushion. Any patient at risk who sits out for more than ½ an hour must be provided with an appropriate cushion Target other pressure relief at vulnerable areas: Dermal Pads for bony prominences such as the spine. Pressure relieving equipment MUST be checked on a shift by shift basis or at each clinical visit to ensure in situ and being properly used. Check inflation of air mattress, check cushions are the right way up, check heel protectors are accessible to the patient and not in a cupboard or on top of a locker. Delays in provision of pressure relieving equipment MUST be reported to the nurse in charge, matron, team leader or senior nurse and a Datix completed. Avoid using footstools – encourage the patient to go back to bed at intervals for limb elevation & pressure relief
Assess Consider all movement, not just turning. Assess both ability to walk and ability to move Assess movement / repositioning requirements when sitting in a chair as well as when lying on a mattress Check the patient’ posture – do they lean to the side when they are seated? Do they have heavy oedematous legs , peripheral vascular disease or neuropathy which might require frequent changes in position of their lower limbs? Heavy oedematous limbs are difficult to move once seated & patients may need a leg lifter as well as heel protection Does the pressure redistributing cushion increase the height of the chair so that the patient’s feet do not touch the floor? This increases the weight put through the buttocks & thighs, raising the risk of pressure damage. You may need to put a foot rise under the patient's feet to ensure their hips, knees & ankles are a 900. Advice to the Patient/Carer Discuss pressure relieving techniques with the patient/carers. Provide the patient information booklet on pressure ulcer prevention & “Tell Us” leaflet . Encourage patients/carers to complete the repositioning documentation Advise patient’s to minimise the time they spend in a seated position, ideally to less than 2 hours. Encourage them to go back to bed for periods in the day to help offload pressure . If the patient has existing sacro-gluteal pressure damage then the time spent seated should be less than 1 hourly intervals Encourage patients to move themselves. Some patients have good upper body strength & can undertake pressure releases when sitting , such as leaning from side to side e.g. paralysed patients . If patients/carers are non-concordant with repositioning advice, try to find out why, document this reason, offer alternative options & inform the Team Leader/Nurse in Charge. If no immediate resolution, complete the Decisions Against Advice form to check no care options are missed. Use verbal reminders to encourage patients to move themselves . The start of TV adverts are a good prompt for some patients
Action Plan an individualised repositioning regime & ensure this links to the risk assessment and specific issues are addressed. Work with patients/carers in the development of this plan Suggest cues for patients to reposition themselves e.g. TV adverts Obtain consent & reposition those patients who are unable to move independently both when in bed & when up in the chair. Use repositioning aids such as slide sheets to minimise shear &friction Consider the 300 tilt Reassess on a regular basis . The frequency will depend on the patient’s condition , level of mobility, results of their skin inspection & level of risk. If there are any changes to any of these factors reassess the patient’s repositioning regime A mobile person during the day may become immobile once in bed, consider an alternating mattress if this cannot be addressed with repositioning. Keep heels floated using heel protection devices Complete the repositioning record each time the patient is repositioned/moved Requires good seating & balance posture & upper body strength
Incontinence increases the level of moisture on the skin and is recognised to be one of the causative factors in the development of pressure ulcers. It increases the risk of friction & the chemical reaction of urine and faeces on the skin causes further tissue breakdown. The ammonia that is produced by this chemical reaction can lead to excoriation of the skin. • Ensure hygiene needs are met. • Wash & thoroughly dry the skin • Use a mild soap or a prescribed skin cleanser. If there are any signs of moisture damage use a specific pH skin cleanser. Perfumed soaps/body washes can irritate the skin that can lead to or exacerbate tissue break down. Do not use baby wipes. • Work with the patient, carers & families to ensure they understand & are able to follow the hygiene regime • Ensure prescribed barrier creams/films are applied as per manufacturer guidelines • Ensure continence products are a good fit and a continence assessment has taken place. • Ask patients, carers and families to complete the “Think SSKIN” chart whenever the opportunity arises.
Encourage a well balanced diet that includes fresh fruit and vegetables, starchy carbohydrates, milk and dairy products and a good source of protein (e.g. meat, eggs, beans etc.). Good nutrition contributes to normal cellular metabolism & fat layers provide a natural padding to protect the bony areas from pressure • Drinking 6-8 drinks a day is advised from a combination of water, juice, squash, tea, coffee and milky drinks. Well hydrated skin will not break down as easily as dehydrated skin. • Carry out MUST screening on admission & regular intervals, but specifically if there are any changes to the patient’s condition. If the patient cannot be weighed then undertake a MUAC • Monitor intake of fluids and food and use food fortification as necessary. • If a patient is undernourished, seek advice from the dietetics team. • Utilise food supplements where appropriate. • Ask patients, carers and families to complete the “Think SSKIN” chart whenever the opportunity arises. • Provide assistance with meals and drinks for those who cannot self care.
D ocumentation Additional Information: Ensure all interventions are evidenced fully & concisely written Reassess care in a timely manner & ensure the care plan reflects changes in clinical condition All grade 2, 3 or 4 pressure ulcers need to be Datixed within 24 hours. All grade 2, 3, or 4 pressure ulcers that are identified as deteriorating in BCHC need to be Datixed within 24 hours Any grade 3 or 4 pressure ulcer that develops in BCHC care needs to be reported as an SI within 48 hours. Bank staff to escalate to the nurse in charge. All grade 3, 4, unstageable pressure ulcers or a deep tissue injury that is not responding to interventions MUST be referred to Tissue Viability via a fax referral form. Any non-concordance in relation to pressure ulcer management MUST be clearly documented along with any alternatives discussed. If non concordance continues and the patient has mental capacity to make the decision, a decision against advice form must be completed by the staff member. It does not require the patient to sign the form. If you are concerned about the condition or safety of a patient escalate this to the Team Leader/Manager & contact the Safeguarding Team
Skin Integrity Cycle • Alter care in accordance with changes – Care Plan • Equipment checks – minimum 3 monthly • Repositioning • Walsall / Waterlow reassessment • Skin inspection • Treatment reassessment • Skin Inspection • Walsall / Waterlowon first contact / with 6 hours of admission • Mobility • MUST • Continence • Grade of PU • Wound assessment • Photo of PU if present • SSKIN Care Plan & Documentation • Continence / Moisture Lesion Care Plan • Nutrition Care Plan • Discuss care with patient, carers & family & give “Think SSKIN” patient information, “Tell Us”, “Talking Leaflets” • Wound Treatment Chart • Regular skin inspection • Mattress, cushion, heel protection • Mobility aids • Repositioning chart & regime • Contact TV G3, G4, unstageable • Datix ( G 2, 3, 4), Contact Risk Management BCHC acquired G 3 & 4