Download
1 / 36
360 likes | 510 Vues
The Role of PTH in Bone Remodeling. Bone Formation. The human skeleton is a flexible, lightweight structural support system for the body. Bones also serve as a reservoir of minerals essential to the proper functioning of every cell in the human body.

E N D
Bone Formation • The human skeleton is a flexible, lightweight structural support system for the body. • Bones also serve as a reservoir of minerals essential to the proper functioning of every cell in the human body. • These minerals are made up of calcium, phosphorus and magnesium. • Through hormonal interplay, these minerals are deposited to or withdrawn from the bones at a moment’s notice to maintain the delicate homeostasis of calcium and phosphorus in the blood.
Types of Bone • The human skeleton is composed of two types of bone: cortical and trabecular. • Cortical bone is also known as compact bone. It forms a protective outer shell around every bone in the body. • Trabecular bone can be found directly beneath the cortical bone. It forms the interior scaffolding that helps bones maintain their shape despite compressive forces.
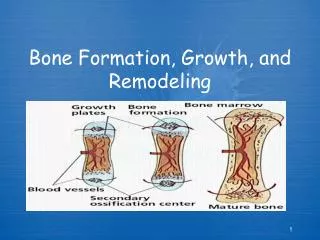
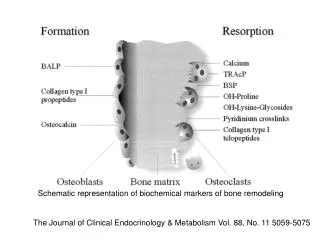
How is Bone Formed? • All bone is formed through the action of bone cells that are distributed sparsely throughout the bone tissue. The two main types of bone cells found are: • Osteoblasts • Osteoclasts ** These have opposite actions and the number of these cells is determined by 1-84 PTH, 7-84 PTH, Vitamin D and estrogen.
Osteoblasts • They are found on the surfaces of newly forming trabecular bone. • When they are completely embedded in the osteoid, they are called “osteocytes”.
Osteoblasts • Osteoblasts build bone; they synthesize and secrete collagen fibrils. The collagen strands combine to form osteoid. • They also cause calcium salts and phosphorus to precipitate from the blood and bond with the newly formed osteoid to mineralize the bone tissue. • Alkaline phosphatase is contained in osteoblasts and is secreted during osteoblastic activity – bone formation.
Osteoclasts • Osteoclasts consume bone. They produce enzymes which break down, or resorb mineralized bone. • Osteoclasts are located • At the sites of bone formation where bone resorption occurs • Throughout the trabecular portion of bone.
Why Does Bone Remodel? • Bone is a living tissue. It is continuously created and re-created by the remodeling actions of osteoblasts and osteoclasts. • Because the bones are constantly under changing stresses and need construction, the remodeling process allows for both the repair of damaged bones and adaptation of bone to different tangential & support stresses. It also facilitates the release of minerals to the blood.
Bone Remodeling • In normal adult bones, the actions of osteoclastic resorption and osteoblastic formation are coupled together – occurring at the same rate – to maintain bone mass at a constant level. • About 10% of bone is replaced through this remodeling process each year.
Bone Remodeling • 1-84 PTH signals osteoclasts to attach themselves and tunnel into the bone, bringing about the resorption of the bone. • Recent data indicates that 7-84 PTH inhibits osteoclast formation and bone resorption. • Osteoblasts are attracted to the cavities and secrete collagen to form osteoid. This is then mineralized to form a new bone layer.
Bone Remodeling • Remodeling begins with the resorption process initiated in part by 1-84 PTH, which signals osteoclasts to attach themselves securely to bone surfaces and tunnel into the bone, bringing about the resorption of the bone. The next step is bone formation. • Osteoblasts are attracted to the new cavities and secrete collagen to form osteoid. This osteoid is then mineralized to form a smooth layer of new bone.
Functions of Calcium • Calcium is the most abundant positively charged ion in the human body (1Kg) and serves many purposes: • Helps form the rigid structure of bone as long, flat, plate-like crystals that are deposited into the bone. • Regulates muscle contraction. • Makes nerve conduction possible. • Facilitates blood clotting – as factor IV, it is necessary to the formulation of thrombin. • Is a cofactor necessary for many enzyme reactions to take place in the body.
Corrected Calcium • Each one gram change in serum albumin per deciliter changes the serum calcium concentration by 0.8 mg/dl. • Normal serum albumin levels range from about 3.5 to 5.0 g/dl. • In patients with below normal albumin levels, obtaining a corrected calcium value can make the difference between recognizing or missing an accurate diagnosis of hypercalcemia.
Calculating Corrected Calcium Albumin Corrected Calcium = Serum calcium + [(4 -albumin) X 0.8] Albumin Corrected Calcium Example: Ca of 10.5 mg/dl & Alb of 2.5 g/dl: = 10.5 + [(4 – 2.5) X 0.8] = 11.7 mg/dl
Calculating Corrected Calcium • Example: Jane Doe has a serum calcium value of 10.5 mg/dl. and a serum albumin of 2.5 g/dl *First, subtract the patient’s albumin value from the low normal albumin value: 4 g/dl – 2.5 g/dl = 1.5 g/dl *Second, multiply the value obtained by 0.8 1.5 X 0.8 = 1.2 *Finally add the results to the patient’s initial serum calcium value 10.5 + 1.2 = 11.7 mg/dl (new calcium value which would correctly lead to a diagnosis of hypercalcemia)
Functions of Phosphorus • Widely available in many foods, phosphorus is vital to energy production and is stored in the bone of the human body. • Is a structural component of fats, proteins and cell membranes. • Stimulates the secretions of selected hormones. • As calcium phosphate, phosphorus is a component of the mineralized crystals of bone. • Normal range should be between 3.5 and 5.5 mg/dl.
PTH • Both 1-84 PTH & 7-84 PTH are synthesized in the four parathyroid glands which are found deep within the thyroid gland. • 1-84 PTH has a half life of 5-10 minutes & 7-84 PTH has a half life of 10-20 minutes. • 1-84 PTH is a protein of 84 amino acids. • 7-84 PTH is a protein of 78 amino acids. • In secondary hyperparathyroidism the parathyroid gland cells enlarge early and the gland enlarges late (hyperplasia) • 1-84 PTH has an amino terminal end at the first amino acid (n-terminal) and a carboxy terminal at the other end or the amino acid #84 (c-terminal).
PTH Regulation of Calcium Homeostasis • PTH (1-84 PTH) has effects on calcium regulation to raise serum calcium through three target organs. • * Effect on kidneys (decreasing Ca excretion) • * PTH stimulates renal tubule resorption to conserve calcium and stimulates the kidneys to produce calcitriol (vitamin D). • Effect on GI tract (increasing Ca absorption) • * PTH increases calcium absorption from the gut indirectly by stimulating the release of vitamin D. This release acts as a feedback mechanism on the glands to shut off PTH secretion.
PTH Regulation of Calcium Homeostasis • Effects on Bones • In the short term, PTH (1-84 PTH) promotes the movement of calcium into the extracellular fluid by prompting the transfer of readily available bone calcium to the extracellular fluid. • In the long term over days or weeks, PTH is secreted in response to chronic hypocalcemia which stimulates osteoclasts and increases bone resorption (to raise serum calcium). • 7-84 PTH lowers serum calcium.
PTH Regulation of Phosphorus Homeostasis *Kidneys • PTH (1-84 PTH) secretion is triggered by high serum phosphorus levels and reduced calcium levels. • PTH reduces renal phosphorus resorption so more phosphorus is removed from the body. * GI • PTH stimulates the production of vitamin D, which increases calcium and phosphorus absorption from the gut. * Bones - PTH increases the solubility of bone calcium by triggering an increased rate of bone remodeling for the release of both phosphorus and calcium into the blood.
Classification of Renal Osteodystrophy • In general there are 4 types of renal osteodystrophy: • Two are classified as “high turnover” • Hyperparathyroid Bone Disease • Mixed Uremic Osteodystrophy • Two are classified as “low turnover” • Adynamic or Low Turnover Uremic Osteodystrophy • Low Turnover Osteomalacia bone disease
Hyperparathyroid Bone Disease • Called “Osteitis Fibrosa”, it is a high turnover disease-- the result of the vicious cycle of secondary hyperparathyroidism. This can be caused by prolonged exposure to high 1-84 PTH levels (with low levels of 7-84 PTH) which increases the overall rate of bone remodeling and alters the structure of the bones. • These are new, soft bones. The cells are high in number, and irregular in shape and arrangement. • Leading to increased fractures and bone pain. • Leading to abnormal soft tissue calcium loads not being absorbed into bones and causing metastatic calcification.
Mixed Uremic Osteodystrophy • Bone remodeling is uncoupled. • Some areas show rapid remodeling like Hyperparathyroid Bone Disease. • Overall the bones are hyperparathyroid, but there are areas with marked accumulations of osteoid as typically observed in Low Turnover Osteomalacia. • Structurally, the bones are weakened, and bone volume is variable.
Low Turnover/Adynamic Uremic Osteodystrophy • The generally accepted cause of this disease is over suppression of 1-84 PTH which can be caused by: • Calcium load (Ca in dialysate bath, Ca containing binder, diet) • Excessive use of vitamin D • Surgical parathyroidectomy • Aluminum overload
Low Turnover Osteomalacia Uremic Osteodystrophy • Without 1-84 PTH, bone remodeling is slow and sparse… • Decreased number of active remodeling sites • Reduced numbers of osteoblasts and osteoclasts • Reduced mineralization • Much of the bone surface is covered with osteoid instead of mineralized bone (i.e. the collagen framework is present without mineralization).
Adynamic Low Turnover Uremic Osteodystrophy • When bone formation has almost completely stopped, the disease is called “Adynamic Uremic Bone Disease”. • When collagen production is normal, but it outpaces mineralization, the condition is called “Low Turnover Osteomalacia.” • In either case, the bones are prone to injury, bowing and fractures.
Aluminum-Related Bone Disease • Caused by exposure to aluminum • Aluminum related bone disease can be superimposed on any of the previous types of bone disease. • Sources of aluminum include under treated water used for dialysate and/or aluminum containing phosphate binders. • Aluminum bonds chemically to the bone itself, interfering with bone cell activity. • Aluminum also interferes with the effects of calcitriol (vitamin D) and PTH – low turnover bone disease • Perhaps more than any other form of renal osteodystrophy, it causes severe, deep bone pain.
Others Effects of Aluminum • Aluminum accumulation also can be responsible for brain injury or dementia in hemodialysis patients, called “Dialysis Encephalopathy.” • Epo-resistant (refractory) Anemia • Bone aluminum cannot be removed by dialysis. • Chelation therapy can be attempted to remove aluminum.
Diagnosis of Osteodystrophy • The later stages of Renal Osteodystrophy, damage to cortical bone may be evident by X-ray. • Subperiosteal resorption • Erosion of the bones of the skull • Bone density cannot be accurately determined by radiography. • Bone mineral density of the spine and/or femoral neck can be semi-quantitated by several methods: • Dual-energy X-ray absorptiometry (DEXA) • Dual photon absorptiometry (DPA) • Double tetracycline labeled bone biopsy is the gold standard for the diagnosis of renal osteodystrophy. Unfortunately, the procedure is invasive and not always easily available.
Ectopic Calcification The calcium x phosphorus product is a measure of the patient’s risk of metastatic calcification. * Levels should be monitored monthly. * A product over 55 indicates an increased risk of this complication. * Even patients receiving vitamin D should always have a product of below 55.
Ectopic Calcification • Deposits of calcium phosphate in the skin which may be one of the factors causing severe Pruritis. • Calcium deposits may occur in nearly any portion of the body. • Different types are: • vascular calcification, periarticular or tumoral calcification, and calciphylaxis.
Vascular Calcification • Calcification may occur in all small and medium-sized arteries and even in the aorta. • A continuous layer of calcium may overlay the vessel walls. • Calcium deposits to these sites can make it difficult to create or maintain vascular access. • On X-ray, the deposits can be seen as a lacy pattern of calcium surrounding the vessels. • It can interfere with successful kidney transplant as there may be no suturable vessels to attach the new organ if the recipient's vesselsare occluded. • If the calcifications are extensive enough to completely occlude blood supply to a region, gangrene can occur.
Periarticular or Tumoral Calcification • When calcium phosphate is deposited into the joints, severe pain, redness and swelling that develop are very much like Arthritis or Gout. “Periarticular calcification” is calcification that surrounds a joint.
Alternative Sites for Calcification • Soft Tissues (extra-skeletal) (calcium deposits almost anywhere) • Kidneys • Heart (arrythmias, CAD, mitral & aortic valves) • Lungs- fibrosis-like restrictive lung disease • Joints
Calciphylaxis • Rare but dangerous consequence of uncontrolled Ca x P product • Calcium deposits to the blood vessels and skin prevent blood flow to the affected areas and cause tissue death. • Typically affects the fingers, toes, ankles or the fat and muscles of the thighs and/or buttocks. • Condition begins as painful, purple mottled areas. • The skin over these areas then ulcerates. • The ulcerations do not heal, Gangrene can occur and the extensive infection can be fatal.