Download
1 / 46
520 likes | 841 Vues
High Altitude Medicine. Scott McIntosh, MD, MPH Director, EMS/Wilderness Medicine Fellowship University of Utah. Connecticut. Why study?. Live in or travel to high areas. Why study?. Live in or travel to high areas Excellent physiology. Why study?. Live in or travel to high areas

E N D
High Altitude Medicine Scott McIntosh, MD, MPH Director, EMS/Wilderness Medicine Fellowship University of Utah
Why study? • Live in or travel to high areas
Why study? • Live in or travel to high areas • Excellent physiology
Why study? • Live in or travel to high areas • Excellent physiology • Expedition medical director
The Plan • Definitions • Acclimatization - by system • Specific problems: • Acute Mountain Sickness (AMS) • High Altitude Cerebral Edema (HACE) • High Altitude Pulmonary Edema (HAPE)
How high is high? 29,000 Extreme 18,000 Very High 12,000 High 8,000 Medium 5,000 Low 0
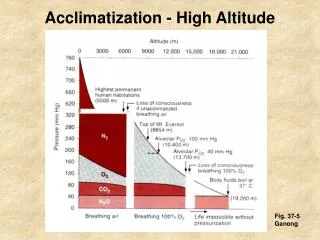
Acclimatization • Definition: series of adaptations the body undergoes when exposed to high altitude for extended periods • Fascinating and complex physiology
Acclimatization schedules Lowlander • Base Camp • To top ice fall then Base Camp • Rest (Base Camp) • Rest (Base Camp) • Base Camp to Camp I • Touch Camp II then back to Camp I • Camp I to Base Camp • Rest (Base Camp) • Rest (Base Camp) • Base Camp to Camp I • Camp I to Camp II • Rest (Camp II) • Part way up Lhotse face then to Camp II • Camp II to Base Camp • Rest (Base Camp) • Rest (Base Camp) • Rest (Base Camp) • Base Camp to Camp II • Rest (Camp II) • Camp II to Camp III • Yellow Band then to Camp II • Base Camp • Wait for weather window
Acclimatization schedules Lowlander • Base Camp • To top ice fall then Base Camp • Rest (Base Camp) • Rest (Base Camp) • Base Camp to Camp I • Touch Camp II then back to Camp I • Camp I to Base Camp • Rest (Base Camp) • Rest (Base Camp) • Base Camp to Camp I • Camp I to Camp II • Rest (Camp II) • Part way up Lhotse face then to Camp II • Camp II to Base Camp • Rest (Base Camp) • Rest (Base Camp) • Rest (Base Camp) • Base Camp to Camp II • Rest (Camp II) • Camp II to Camp III • Yellow Band then to Camp II • Base Camp • Wait for weather window Sherpa • Base Camp • Base Camp • Base Camp • Base Camp • Base Camp • Base Camp to Camp II • Rest (Camp II) • Base Camp • Base Camp • Wait for weather window
Respiratory • Hypoxic Ventilatory Response • Carotid bodies sense decreased pO2 • Central medullary receptors sense pH changes (CO2 diffuses across, dropping pH) • Response is genetically predetermined • South American vs. Himalayan natives
Hypoxic Ventilatory Response Am J Phys 1949 157:445-62
Acid-Base Changes • Result: mild resp alkalosis approx 7.48 (blowing off CO2) • After 1-2 days: Kidneys respond with H+ conservation and HCO3- excretion • pH restored close to (but not = to) 7.40 (occurs at approx 1 week)
Circulatory System • Sympathetic Stimulation: • Increased HR, BP, inotropy • Selective vasoconstriction (muscles, skin, viscera) • SNS normalizes during acclimatization Am J Cardiol 1990 (Operation Everest II) 65:1475-80
Hematological System • Hypoxia causes erythropoietin release • HCT usually 30% above sea level • HCT’s above 75% not uncommon
Help Acclimatization • Graded Ascent • More difficult-easy to travel eg: Lukla • Fluids, high CHO diet • Younger • more susceptible • Physically fit • no protection
Help Acclimatization • Vitamin C • Calcium Ascorbate • Siberian Ginseng extract • L-Tyrosine • Ginkgo Biloba extract • Schizandra extract • Ginger Root extract • Reishi Mushroom extract
Help Acclimatization • Diamox • causes renal bicarb excretion leading to metabolic acidosis, increasing ventilation • diuretic action decreases edema • sulfa drug and side effects CO2 + H2O H2CO3 H+ + HCO2- Carbonic Anhydrase
AMS • Headache plus at least one of the following: • GI upset, weakness/fatigue, difficulty sleeping, dizziness or light-headedness • Nausea, vomiting, anorexia common
AMS • Symptoms develop within a few hours • Max intensity at 24-48 hours • Symptom free at day 3-4 Aviat Space Environ Med 1980;51:872-77
General Treatment of HA Problems • Descent • Portable hyperbaric chamber • Oxygen • Specific medications
Characteristics Treatment
High Altitude Cerebral Edema • Continuum of AMS • Brain swelling • Hallmark symptoms: • Ataxia, mental status changes, confusion, stupor, coma
HACE - Treatment • Early recognition required • Mandatory descent and evacuation • All general high altitude illness treatments • Dexamethasone 8 mg IM or IV then 4 mg every 6 hours • Prognosis good to deadly
HAPE • Most common cause of death in HA • Non-cardiogenic pulmonary edema • At 14K on Denali: • O2 sats in 56% • Avg pO2 = 28 J Appl Physiol 64:2605,1988
HAPE Physiology • Normally hypoxia/ischemia produces vasodilation • In lungs, HYPOXIC VASOCONSTRICTION
HAPE CXR • Patchy b/c of different areas of hypoxia and vasoconstriction, relocation of blood and therefore edema • Normal heart • No Kerley lines
HAPE Susceptibility • People who have abnormally high PAP • Possibly congenital reduced NO synthetase
HAPE Treatment • Oxygen and descent usually sufficient • If those not available, nifedipine • Decreases pulmonary hypertension • New drug?
High Altitude Medical Kit • Meds: • Diamox – PO • Nifedipine – PO • Dexamethasone – IV • Ginko? • Oxygen? • Gamow bag?