Download
1 / 29
350 likes | 715 Vues
High-Altitude Medicine. Alicia Bond MD. High altitude. Moderate altitude 5,000 – 10,000 feet above sea level Highest U.S. ski resorts High altitude 10,000 – 18,000 feet above sea level High peaks in the lower 48, Europe Extreme altitude Greater that 18,000 feet above sea level

E N D
High-Altitude Medicine Alicia Bond MD
High altitude • Moderate altitude • 5,000 – 10,000 feet above sea level • Highest U.S. ski resorts • High altitude • 10,000 – 18,000 feet above sea level • High peaks in the lower 48, Europe • Extreme altitude • Greater that 18,000 feet above sea level • Denali, Himalaya, Karakoram, Andes
Epidemiology • Most cases of high-altitude illness take place in people rapidly ascending to altitudes between 8,000 and 12,000 feet • Can affect people who live at low altitude as well as people who live at high altitude and return from travel to lower altitude (re-entry) • Millions at risk each year – roughly 20-40% affected by some type of altitude illness • 30 million Western states visitors • 12,000 Mt. Everest trekkers • 1,200 Denali climbers • 1 million visitors to extreme high ranges worldwide
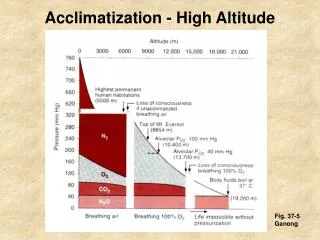
High-altitude environments • Decreased barometric pressure = logarithmically lower partial pressure of oxygen (PO2) in inspired air • Higher latitudes have lower barometric pressure at equivalent altitudes • Weather systems can significantly lower barometric pressure transiently • Cold, dry conditions may be contribute to high-altitude illness
Factors affecting risk • Rate of ascent • Recent high-altitude exposure • Genetic variability • Sleeping altitude • Maximum altitude reached
Acclimatization • Series of physiologic adaptations to maintain tissue oxygenation • Ability to acclimatize varies genetically • Hours: Hypoxic ventilatory response (HVR), fluid shift to increase hematocrit, increase in cardiac output • Days: Increased erythropoiesis, return of cardiac function to baseline, increase in 2,3-DPG • Weeks: Increased plasma volume and red blood cell mass
Hypoxic ventilatory response • Most important component of acclimatization • Affected by genetics, ethanol, sleep medications, caffeine, cocoa, progesterone • PaO2 = PiO2 (PaCO2/R) • Hyperventilation decreases the partial pressure of CO2 in the alveoli, thereby increasing the partial pressure of oxygen in the alveoli to facilitate oxygenation • Resulting metabolic alkalosis slows HVR, and ventilation slowly increases over several days as kidneys excrete bicarb • Can be facilitated by acetazolamide • People with low HVR at higher risk for illness
Cardiovascular • Initial increase in resting HR, which normalizes with acclimatization • Decrease in maximal heart rate • Decrease in plasma volume -> lower stroke volume, increase in hematocrit • Shift to extracellular space • Diuresis from bicarbonate excretion • Decrease in max HR and SV are cardioprotective – myocardial ischemia is rare
Hematopoietic response • Initial increase in hematocrit due to fluid shift and diuresis • Erythropoietin stimulated early, resulting in new RBCs within 4-5 days • Over weeks to months, red cell and total circulating volume expand to meet demand
Oxygen-hemoglobin curve • Above 10,000 feet (PO2 ~ 60), small changes in PO2 cause large changes in SaO2 • Initial increase in 2,3-diphosphoglycerate (DPG) promotes O2 release to tissues • Opposed by respiratory alkalosis, which shifts curve left, favoring oxygen uptake in the lung and higher SaO2
Sleep and periodic breathing • Disturbed sleep with less deep sleep and significant arousals common • Periodic breathing common • Hyperpnea and respiratory alkalosis cause apnea • CO2 builds during apnea, causing hyperpnea • Not usually associated with significant hypoxemia or high-altitude illness • Decreases with acclimatization • People with low HVR may have overall regular breathing pattern with periods of more significant apnea and hypoxemia, which are associated with high-altitude illness
Acute high-altitude illness • Spectrum of disease with intertwining pathophysiology • Acute mountain sickness (AMS) • High altitude cerebral edema (HACE) • High altitude pulmonary edema (HAPE) • All correct rapidly with descent
Prevention of high-altitude illness • Avoid ascent to greater than 8,000 feet in one day • Spend 2-3 nights at 8,000-9,000 feet before further ascent • Don’t ascend sleeping altitude more than 1500 feet per day • Limit exertion, alcohol, and sedative-hypnotics during first days at altitude • Day trips to higher altitude while maintaining sleeping altitude can speed acclimatization • Acetazolamide 125-250 mg BID
Acute mountain sickness • Most common with rapid ascent from below 3,000 feet to above 8,000 feet • Develops within hours of ascent • Headache plus at least one of: • Gastrointestinal discomfort • Sleep disturbance • Generalized weakness or fatigue • Dizziness or lightheadedness • Headache is usually throbbing, bitemporal, worse at night and with Valsalva
AMS: Pathophysiology • Pathophysiology incompletely understood • Vasodilatory response to hypoxemia, fluid shift, inflammatory mediators, and alterations in cerebrospinal fluid buffering capacity are all implicated • No evidence of cerebral edema in AMS, but some studies suggest transient ICP elevations with exertion and Valsalva • At risk may be people with low HVR and people with smaller CSF capacity (“tight fit”) • Hyperbaria contributes, but role unclear (AMS does not develop with hypoxia alone)
AMS: Management • Usually resolves within 1-3 days if no additional ascent • Mild: Stop ascent, symptomatic treatment, may consider acetazolamide • Moderate to severe: Low-flow oxygen, acetazolamide +/- dexamethasone 4 mg q 6 hours, hyperbarics, or descend • Immediate descent if s/sx HAPE or HACE
Acetazolamide • Carbonic anhydrase inhibitor • Promotes bicarbonate diuresis and metabolic acidosis, speeding acclimatization • Decreases CSF production • Maintains oxygenation during sleep • Side effects: polyuria and paresthesias • 125-250 mg BID for treatment and prevention of AMS
High-altitude cerebral edema • Least common but most severe form of high-altitude illness • Incidence 1-2% of ascents • Usually develops above 12,000 feet • Usually preceded by AMS and associated with HAPE • Most commonly develops days 1-3 after ascent, but can develop later
HACE: Presentation • Ataxia and altered mentation are hallmarks – ataxia usually first symptom • Focal neuro deficits may be present • Seizures uncommon but reported • Usually preceded by AMS symptoms • Any ataxia or change in consciousness in a person at altitude should elicit immediate action!
HACE: Pathophysiology • Vasogenic cerebral edema caused by same group of mechanisms as AMS (vasodilation, leakage of fluid from vessels) – reversible • Increased ICP causes decreased cerebral blood flow, resulting in cell death • At advanced stages, cytotoxic edema and necrosis are present - not reversible
HACE: Management • Immediate descent is key • High-flow oxygen and dexamethasone 8 mg (IV, IM, PO) followed by 4 mg q 6 hours if available • Hyperbarics may result in temporary improvement but may delay descent • Intubation, hyperventilation if severely altered • Can try mannitol or furosemide but caution due to dehydration common at altitude
HACE: Prognosis • If descent initiated early, may be completely reversible over days to weeks without sequelae • Reports of ataxia and other neuro deficits persisting months to years • Mortality rate greater than 60% if progresses to coma
High-altitude pulmonary edema • Most common cause of altitude-related death • Incidence up to 15% of ascents • Usually greater than 10,000 feet, or greater than 8,000 feet with heavy exertion • Develops within 2-4 days of ascent, classically on the second night
HAPE: Presentation • Early signs are severe dyspnea on exertion, fatigue with minimal activity, and dry cough • Dyspnea at rest and clear, watery sputum develop as illness progresses • Dyspnea at rest is red flag for HAPE and should prompt immediate action! • Patchy infiltrates on CXR, worst right middle lobe
HAPE: Pathophysiology • Hypoxic vasoconstriction causes pulmonary hypertension • Uneven vasoconstriction (areas of extreme hypoxia or anatomic difference) causes hyperperfusion of some areas, leading to vascular leak and patchy edema • Both hypoxia and pulmonary hypertension are exacerbated by exertion
HAPE: Management • Symptoms resolve quickly upon descent of 1500-3000 feet • Mild cases may be treated with bedrest and O2 to maintain SaO2 > 90 • Descent for severe symptoms, minimizing exertion • High-flow oxygen • Continuous positive airway pressure if available • Air drops of O2 may be lifesaving if descent not possible • Hyperbarics may help conserve O2 supply
Hyperbarics • Portable, lightweight,manually-pressurizedhyperbaric bags • Raise atmospheric pressure 2 psi (103 mmHg) • Simulates descent of 4,000-5,000 feet at moderate altitudes, more at higher altitudes • Can be lifesaving in HAPE and HACE, relieving symptoms so that patients can descend without evacuation Photo: Rosen’s Emergency Medicine, Courtesy of Thomas Dietz, MD
Take-home • Slow ascent and acetazolamide are effective in preventing illness • Ataxia, altered mentation, and dyspnea at rest are red flags for serious illness • Early recognition of HAPE and HACE with descent prevents morbidity and mortality • Have fun up there!
Key References • Marx, JA, ed. Rosen’s Emergency Medicine, 7th Ed. Philadelphia: Mosby Elsevier, 2010 • Auerbach, PS, ed. Wilderness Medicine, 6th Ed. Philadelphia: Mosby Elsevier, 2012