Download
1 / 48
480 likes | 633 Vues
HYPERSENSITIVITY REACTIONS. HYPERSENSITIVITY REACTIONS Innocous materials can cause hypersensitivity in certain individuals. unwanted inflammation damaged cells and tissues. Non-proper reaction of the immune system to foreign substances

E N D
HYPERSENSITIVITY REACTIONS Innocous materials can cause hypersensitivity in certain individuals unwanted inflammation damaged cells and tissues Non-proper reaction of the immune system to foreign substances Mainly harmless substances – after second or multiple times
TYPES OF HYPERSENSITIVITY REACTIONS mostly appear together with autoimmune diseases
TYPES OF HYPERSENSITIVITY REACTIONS Hay fever Asthma Systemic anaphylaxis Certain drug allergies (penicillin) Serum sickness Arthus reaction
TYPE I HYPERSENSITIVITY REACTION ALLERGY
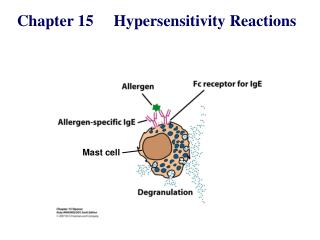
ALLERGENES USUALLY ENTER THE BODY VIA MUCOSAL SURFACES AND THEY ARE PRESENT AT A LOW DOSE DC Th2 Th2 allergy response B cell antigen presentation T cell priming and polarization • soluble proteins on te surface of small particles (pollen, dust mite „drops”) • small Mol. Weight, soluble • trans mucosal entry, enzymatic activity • low dose (ragweed: 1µg/year)
Mechanism of the initiation of Th2 response IL-4 CD4+ T IL-4 IL-10 Allergen Mucosa
Mast cell degranulation, wheel and flare reaction Ragweed Saline Histamine
MAST CELL RESPONSE TO SURFACE FcRεI CROSSLINKING EARLY MEDIATORS Biognic amins – histamin Enzymes – triptase, chymase, carboxypeptidase LATE MEDIATORS
The effect of mast cell degranulation varies with the tissue exposed to allergen
Systemic anaphylaxis is caused by allergens that reach the blood stream
GENETIC/ENVIRONMENTAL PREDISPOSITION TO ALLERGY Genetic factors chromosome 11q FcERβ chain gene chromosome 11q IL-3-5 IL-9, IL13 GMCSF HLAII DRB1*150 Improper immunregulation Th1/Th2 inbalance regulation of IgE synthesis immunodeficiency high eosinophil counts Environmental factors lack of tolerance allergy
Short/Common ragweed (Ambrosia artemisiifolia) Mugwort (Artemisia vulgaris) levélfonák zöld levélfonák fehéresen molyhos
Mugwort (Artemisia vulgaris) – ? Wormwood (Arthemisia absinthium) – Absinthe (thujone: max 35 mg/l)
HYPERSENSITIVITY REACTIONS INDUCED BY IMMUNE COMPLEXES TYPES II and III • cells expressing the antigen become sensitive to complement mediated lysis or to opsonized phagocytosis • frustrated phagocytosiss tissue demage • the antibody inhibits or stimulates target cell function • no tissue damage (e.g. M. gravis – receptor blocker antibodies) Type II hypersensitivity IgG tpye antibodies bound to the cell surface or to tissue antigens
MECHANISMS OF TYPE II HYPERSENSITIVITY REACTIONS Hemolytic anemia of newborns Erythroblastosis fetalis Drug induced Hemolytic anemia Trombocytopenia Agranulocytosis Penicillin-based antibiotics Anti-arythmic quinidin Goodpasture syndrome (type IV collagen) Pemphigus vulgaris (desmosomal antigens) Damage of epidermal and mucosal junctions, acantholysis
Th B MECHANISM OF THE DEVELOPMENT OF DRUG SENSITIVITY Drug-modified cell surface protein Healthy cell IgG type antibodies
FRUSTRATED PHAGOCYTOSIS MEDIATED BY IgG TYPE ANTIBODIES Binding Opsonization Internalization Enzyme release The tissue, which can not be phagocytosed, is damaged Internal or absorbed antigen (drug) Opsonized surface Binding Frustrated Enzyme release phagocytosis
Examples - Type II hypersensitivity Newborn haemolytic anaemia Transfusion reaction Hyperacut allograft rejection Drug-derived • Haemolitic anaemia • Thrombocytopenia • Agranulocitosis • Penicillin-based antibiotics • Anti-arithmic quinidin Goodpasture syndrome (kidney, membrane basalis, collagen type IV) Myasthaenia gravis (anti-acetyl-choline receptor antibodies) Basedow-disease (anti-TSH-receptor antibodies) Pemphigus vulgaris (mucosal bubbles) atoantibody against desmosomal antigen desmoglein-3, interruption of epidermal and mucosal connections, acantolysis (disintegration into single cells)
HLA-A, B, C, DR, DQ, DP, minor histocompatibility antigens foreign MHC-antigens recognized by T cells Direct: self T cells - donor APCs (CD8+ T cells) Indirect: self APC presents donor MHC-molecule fragments (CD4+ T cells) cytokine release Hyperacut rejection Causes: immunization against alloantigens, preformed anti-HLA-antibodies, blood group incompatibility antibodies bound to endothel activation of complement system thrombosis of venules vascularis necrosis Therapy resistent Transplantation - hyperacut allograft rejection
HLA typing MHC I: HLA-A, HLA-B, HLA-C MHC II: HLA-DP, HLA-DQ, HLA-DR • used for transplantations • (generally the -B and -DR is the most important and the -C does not matter) • diagnostical value • (connections between the HLA alleles and the diseases) Serotyping(microcitotoxicity tests) Based on the serological reaction between the examined cells and the typing serum. Complement mediated lysis with the help of MHC I and/or MHC II antigen recognizing antibody containing serum. There are no reaction in the case of serotype identity (dead cells can be visualized by specific dye) Typing sera containing antibodies to Class I and II proteins were collected from multiparous women, or individuals who had received multiple blood transfusions. (immunized against multiple alleles). The specificity identification have been done on international workshops. The procedures have been done on microtiter plates (with 10µl working aliquots – Terasaki plates) because of the available quantity of the typing sera were always limited. Sera have been replaced by monoclonal antibodies later.
Serotyping (2.) HLA-D (MHC II) antigenes had been examined on nylon column separated B cells The polymorphism of the MHC II antigens could be examined by mixed lymphocyte reactions (MLR). (A normal person can have 1-10% alloreactive lymphocytes.) Microtiter plates
serotyping have some limits – crossreactions (HLA-B27 – HLA-B7) – there is no sera against HLA-C because of the low immunogenicity – some subtype cannot be discriminated HLA-A 0201 0202 0203 … Genomic DNA based examinations • PCR-SSP is using the PCR amplification reaction directly to detect HLA polymorphisms. Primers can be constructed specifically to complement HLA polymorphisms; if the primers bind the complementary polymorphism and amplify the gene segment, then the PCR product can be detected by standard techniques. An array of PCR primers complementary to the range of HLA polymorphisms has been constructed.
PCR-SSOP (sequence specific oligonucleotid probe) • The examined HLA genes are amplified by PCR with non allele specific primer pairs. The amplificates are immobilized on nitrocellulose membranes or microtiter plates and are hybridized by HLA allele specific labeled oligonucleotides. • The label can be enzimatic, fluorescent or radioactive • SBT(sequence based typing) • allotypes can be evaluated by sequencing MHC region of the genomic DNA • (minor mutations can be examined)
HLA allotypes and diseases ref: Klinikai immunológia (II. klinikum) (OHVI 1990 szerk.: Szegedi, Gergely, Sipka, Szemere) Stenszky Valéria: Autoimmun betegségek genetikai vonatkozásai
HLA-A alleles described until october 2006 http://www.ebi.ac.uk/imgt/hla/allele.html
Type IV hypersensitivity reaction Chemokines, cytokines, cytotoxins
Delayed-type Hypersensitivity (Type IV Hypersensitivity)
Delayed-type Hypersensitivity (Type IV Hypersensitivity)
Delayed-type hypersensitivity (DTH) (e.g., tuberculin skin test) TH1 from a previous immunization (memory)
DTH as a result of a contact-sensitizing agent* Contact Dermatitis *a contact-sensitizing agent is usually a small molecule that penetrates the skin then binds to self-proteins, making them “look” foreign
Poison ivy Anacardiaceae (family), Toxicodendron (genus) Toxicodendron radicans or Rhus toxicodendron
Delayed-type hypersensitivity is mediated by T cells (Type IV hypersensitivity)
Delayed-type Hypersensitivity A positive tuberculin skin test is a DTH reaction
TYPE III HYPERSENSITIVITY Antibodiesbinding to solubleantigens Small circulating immune complexes Depends on: Size of immune complexes Antigen-antibody ratio Affinity of antibody Isotype of antibody
THE PROCESS OF TISSUE DAMAGE CAUSED BY IMMUNE COMPLEXES Blood vessel wall permeability Frustrated phagocytosis Immune complexes activate the complement system, neutrophils, bazophil granulocytes and thrombocytes
ANA Anti -nuclear antibody