Download
1 / 57
630 likes | 1.13k Vues
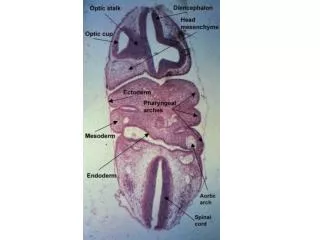
Infection of pharyngeal spaces. Retropharyngeal Space Infection. The retropharyngeal space lies behind the pharynx and esophagus, just anterior to the prevertebral fascia. It extends superiorly to the base of the skull and inferiorly to the bifurcation of the trachea.

E N D
Retropharyngeal Space Infection • The retropharyngeal space lies behind the pharynx and esophagus, just anterior to the prevertebral fascia. It extends superiorly to the base of the skull and inferiorly to the bifurcation of the trachea. • Patients generally present with trismus, drooling, dyspnea, dysphagia, and a mass, often fluctuant, on one side of the posterior pharyngeal wall. • Lateral radiographs of the neck are also helpful in diagnosis. It is important, however, to have proper positioning of the patient at the time of X-ray; otherwise the results may be misleading. The patient should have the neck extended in a true lateral position for the X-ray.
Parapharyngeal Space Abscess • The parapharyngeal space is cone shaped. Superiorly it starts at the base of the skull and inferiorly its margin ends at the hyoid bone. The superior constrictor muscle is the medial boundary, and the parotid gland, the mandible, and the pterygoid muscle are its lateral margins , the prevertebral fascia is present posteriorly. • A parapharyngeal space abscess can develop when infection or pus from the tonsillar region goes through the superior constrictor muscle. The abscess then forms between the superior constrictor muscle and deep cervical fascia. • Patients can present with toxemia and pain in the throat and neck, with tender swelling of the neck in the region of the angle of the mandible. Examination may reveal tonsillitis and/or medial displacement of the tonsil.
Parapharyngeal Abscess Retro-pharyngeal Abscess (Acute & Chronic) Infection of Pharyngeal Spaces
Parapharyngeal Abscess Collection of pus in the PARA-PHARYNGEAL Space Def What is parapharyngeal space? • A connective tissue space which: • Lies on the lateral side of the nasopharnx and oropharynx • Extends from skull base to hyoid bone • Contains: • Internal carotid artery • Internal jagular vein • Last 4 cranial nerves • Cervical sympathetic trunk • Deep cervical lynph nodes
The infection passes through the Superior constrictor muscle Etiology: • Acute Tonsillitis or after tonsillectomy • Infection of last lower molar tooth • Infection of the parotid salivary gland Symptoms Same as in Quinsy
- The lateral pharyngeal wall & tonsil is pushed medially - Trismus due to spasm of ptrygoid muscles Signs: General; fever Pharyngeal: Cervical Investigations: CT & MRI • A unilateral diffuse tender swelling : • Below & behind the angle of the mandible • Deep to the anterior border of the sternomastoid • The neck is tilted to the diseases side
Complications Spread to - Skull base meningitis carotid sheaththrombosis of IJV and rupture of carotid artery Mediastinum Mediastinitis Larynx laryngeal edema Ruptureinto the pharynx aspiration Bronchopneumonia
Treatment Medical: massive antibiotic therapy and, Surgical drainage Sternomastoid A vertical incision at the anterior border of the sternomastoid muscle
Collection of pus in the retropharyngeal space Acute Retropharyngeal Abscess • It is a connective tissue space between : • the buccopharyngeal fascia & pre-vertebral fascia • The two fasciae are attached to each side by median raphe. • It extends from the skull base to the posterior mediastinum • It contains retropharyngeal lymph node one on each side • The Retropharyngeal LN atrophy at the age of 5 BuccoPharyngeal Fascia The Retropharyngeal space Prevertebral fascia
Age: below the age of 5 (The Retropharyngeal LN atrophy at the age of 5) Site: at one side of the midline (The two fasciae are attached to each other at the midline by median raphe.) Etiology Upper Rrspiratory Tract Infection with suppuration of Retropharyngeal LN After Adenoidectomy operation Impacted FB
Symptoms In A child below 5 years General: FHAM Pharyngeal: Severe sore throat Dysphagia Difficult breathing Abscess
Signs General: fever Pharyngeal Swelling of the posterior Pharyngeal wall to one side of the midline Cervical: Neck inclination due to muscle spasm
Normal PatientLateral view of the Neck • Look for • The vertebral column ( for any destruction e.g in Pott’s disease) • The pre-vertebral space(3/4 the width of the body of the vertebra) • The airway
Investigations: plain X ray & CT scan • Complications: • Spread to mediastinummediastinitis • Rupture…………. Widening of prevertebral space Normal vertebral bodies
Treatment Medical: massive antibiotic therapy and, Surgical drainage Tracheostomy if indicated Incision in the posterior pharyngeal wall with the patient in the Trendlenberg position Why? In this position the head is lower than the chest to avoid aspiration of pus
Chronic Retropharyngeal AbscessPre-vertebral Abscess What is the pre-vertebral space? A space between: • The cervical vertebrae • The pre-vertebral fascia Formation of a cold abscess in the pre-vertebral space
Etiology: Pott’s Disease i.e tuberculosis of cervical vertebrae the abscess rupture through the prevertebral fascia the abscess reaches the Retropharyngeal space prevertebral fascia
Symptoms In an adult General: Tuberculous Toxaemia Pharyngeal: Mild sore throat Cervical: limited painful neck movement -Night sweets -Night fever -Loss of weight -Loss of appetite
Signs: General: Tuberculous toxaemia Pharyngeal: Cervical: Tenderness over cervical spines Pallor Low grade fever Loss of weight The swelling lies in the midline of the posterior pharyngeal wall
Investigations Plain X ray & CT scan Widening of the Prevertebral space Destruction of the cervical vertebrae
Treatment: Medical: Antituberculous therapy Surgical Drainage Orthopedic Management Through a vertical incision along the posterior border of the sternomastoid muscle
Synonyms • Hypopharyngeal diverticulum • Zenker’s diverticulum • Pharyngo-oesophageal pouch • Retropharyngeal pouch • Killian’s diverticulum
Introduction • Hypopharyngeal pouch is an acquired pulsion diverticulum caused by posterior protrusion of mucosa through pre-existing weakness in muscle layers of pharynx or esophagus. • In contrast, congenital diverticulum like Meckel's diverticulum is covered by all muscle layers of visceral wall.
Weak spots b/w muscles Posterior: 1. Between Thyropharyngeus & Crico- pharyngeus: Killian's dehiscence (commonest)
History • First described in 1769 by Ludlow • Friedrich Zenker & von Ziemssen first described its picture in their book in 1877
1. Tonic spasm of cricopharyngeal sphincter: C.N.S. injury Gastro-esophageal reflux 2. Lack of inhibition of cricopharyngeal sphincter 3. Neuromuscular in-coordination between Thyro-pharyngeus & Cricopharyngeus 4. Second swallow against closed cricopharynx These lead to increased intra-luminal pressure in hypopharynx & mucosa bulges out via weak areas.
Entrapment of food in pouch: sensation of food sticking in throat & later dysphagia • Regurgitation of entrapped food: leads to foul taste bad odor nocturnal coughing choking • Hoarseness: due to spillage laryngitis or sac pressure on recurrent laryngeal nerve • Weight loss: due to malnutrition • Compressible neck swelling on left side: reduces with a gurgling sound (Boyce sign)
Complications • Lung aspiration of sac contents • Bleeding from sac mucosa • Absolute oesophageal obstruction • Fistula formation into: trachea major blood vessel • Squamous cell carcinoma within Zenker diverticulum (0.3% cases)
Investigations • Chest X-ray: may show sac + air - fluid level • Barium swallow • Barium swallow with video-fluoroscopy • Rigid Oesophagoscopy • Flexible Endoscopic Evaluation of Swallowing
Introduction • Normal length of styloid process is 2.0–2.5 cm • Length >30 mm in radiography is considered an elongated styloid process • 5-10% pt with elongated styloid have pain • Increased angulation of styloid process both anteriorly & medially, can also cause pain • Commonly seen in females over 40 years.
Classical Variety • Occurs several years after tonsillectomy • Pharyngeal foreign body sensation • Dysphagia • Dull pharyngeal pain on swallowing, rotation of neck or protrusion of tongue • Referred otalgia • Due to scar tissue in tonsillar fossa engulfing branches of glossopharyngeal nerve
Theories for pain • Irritation of glossopharyngeal nerve • Irritation of sympathetic nerve plexus around internal carotid artery • Inflammation of stylo-hyoid ligament • Stretching of overlying pharyngeal mucosa
Diagnosis • Digital palpation of styloid process in tonsillar fossa elicits similar pain • Relief of pain with injection of 2% Xylocaine solution into tonsillar fossa • X-ray neck lateral view • Ortho-pan-tomogram (O.P.G.) • Coronal C.T. scan skull • 3-D reconstruction of C.T. scan skull