Download
1 / 50
500 likes | 674 Vues
Allocation of deceased donor kidneys. Phil Clayton NSW Renal Group 14 June 2012. Outline. Why study kidney allocation? Equity vs utility Current Australian model Previous work in Australia US allocation research Allocation simulations Current model A utility-based model

E N D
Allocation of deceased donor kidneys Phil Clayton NSW Renal Group 14 June 2012
Outline • Why study kidney allocation? • Equity vs utility • Current Australian model • Previous work in Australia • US allocation research • Allocation simulations • Current model • A utility-based model • Future directions
Equity vs utility trade-off • Equity • Everyone has opportunity to benefit from transplantation • Utility • Get most out of precious resource • Patient survival • Graft survival • QALYs? • Cost effectiveness?? • Whose perspective? • Patient / Donor / System / Society
Current Australian model • Major listing criteria: • ESKD on dialysis • 80% likelihood of surviving for at least 5 years after transplantation • Major allocation criteria: • Blood group Equity/Utility • Waiting time Equity • HLA match Utility • Highly sensitised Equity/Utility • Childhood Utility
Other states • VIC – HLA-B, -DR, waiting time • SA – HLA-A, -B, -DR, waiting time • QLD – HLA-A, -B, -DR, waiting time, paediatric status • WA – HLA-A, -B, -DR; HLA-DR homozygous; waiting time
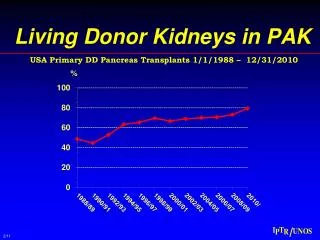
Young donors Old patients Old donors Young patients
More benefit from age matching if higher proportion of older donors
US allocation research • Extensive modelling and simulations • Proposed algorithm: • Scores for kidney donors and wait-listed patients • Top 20% kidneys -> top 20% recipients • Other 80% kidneys -> recipients aged within 15 years of donor
Allocation simulations Waiting list Simulation software Allocation algorithms Donor pool • Outcomes • Equity of access • Utility • Patient survival • Graft survival • ? others
NOMS-ANZDATA link • NOMS • National database of kidney allocation • Since 2000 (Y2K) • Detailed waiting list data since 28 June 2006 • Data extract 2001-2010 • Demographics, serology, antibodies, crossmatch results, organ match results • Probabilistic linkage with ANZDATA
Simulation modelling • Visit to Ann Arbor, Michigan • Great people • Spring snow (new jacket) • Bad coffee • Simulation software • Developed for US • Adapted for ANZDATA/ANZOD/NOMS data • Australia allocation rules • Validation against actual allocation
Utility-based allocation • Factors affecting transplant benefit • Age • Sex • Race • Primary disease • Co-morbidities • Diabetes • Coronary disease • Peripheral vascular disease • Cerebrovascular disease • Chronic lung disease • Smoking history • Body mass index • Time on RRT • Waiting time • Donor age • Ischaemic time • HLA mismatch • Peak PRA
Utility-based allocation • Factors affecting transplant benefit • Age • Sex • Race • Primary disease • Co-morbidities • Diabetes • Coronary disease • Peripheral vascular disease • Cerebrovascular disease • Chronic lung disease • Smoking history • Body mass index • Time on RRT • Waiting time • Donor age • Ischaemic time • HLA mismatch • Peak PRA Benefit = 26 – (age/4) - (donor age/20) - (HLA mismatch/3) - (peak PRA/20)
Future directions • More sophisticated allocation models • Sensitivity analyses • Changes in waiting list • Changes in donor pool • QALYs • Economic analyses
Acknowledgements • ANZDATA • Blair Grace • Stephen McDonald • Steve Chadban • NOMS • Jeremy Chapman • Jenni Wright • Paul Slater • Arbor Research Collaborative for Health • Keith McCullough • Bob Merion • Alan Leichtman • Australian and New Zealand patients and staff for their cooperation and contributions to ANZDATA and ANZOD