Download
1 / 1
10 likes | 115 Vues
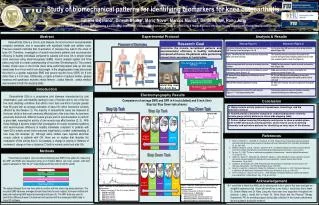
This research investigates muscle recruitment patterns and neuromuscular efficiency in patients with knee osteoarthritis compared to healthy individuals during closed-chain exercises. Using electromyography (EMG), motion analysis, and force plates, this study explores how knee osteoarthritis develops. Findings show higher EMG and ground reaction force for greater step height. Understanding these patterns can lead to better management and treatment for knee osteoarthritis.

E N D
Study of biomechanical patterns for identifying biomarkers for knee osteoarthritis Tatiana Bejarano1, Dinesh Bhatia1, Mario Novo2, Marcos Munoz2, Denis Brunt2, Ranu Jung1 1Adaptive Neural Systems Lab, College of Engineering & Computing: Department of Biomedical Engineering, 2College of Nursing & Health Sciences: Physical Therapy Department , Florida International University. Analysis & Results Abstract Experimental Protocol Osteoarthritis (OA) is a chronic joint disease, the most common musculoskeletal complaint worldwide, and is associated with significant health and welfare costs. Previous research indicates that co-activation of muscles may lead to the onset of knee OA. Therefore, investigation of muscle recruitment patterns and neuromuscular efficiency in healthy individuals compared to patients with knee OA in simple closed chain exercises using electromyography (EMG), motion analysis system and force plates may lead to a better understanding of how knee OA develops (6). The present studies chosen were in the frontal plane while performing lateral step up and step down tasks for a 4 inch and 8 inch step height. In the stepping tasks it was discovered that there is a greater magnitude EMG and ground reaction force (GRF) for 8 inch rather than a 4 inch step. Additionally, a higher activation of gluteus medius, gluteus maximus and quadriceps muscles (rectus femoris , vastuslateralis , vastusmedius) was revealed in both the stepping tasks. Placement of Electrodes Lateral Step down from 8 inch Step Introduction Electromyography Results Osteoarthritis (OA) is a progressive joint diseases characterized by joint inflammation, pain and disability leading to loss of function and is one of the top five most disabling conditions that affects more than one-third of people greater than 65 years with an average estimation of about 30 million Americans currently affected by this disease (1). The majority of osteoarthritis cases are observed at the knee, which is the most commonly affected joint of the lower limb. As has been previously discovered, different muscle groups work in synchronization to perform a given task, meaning the activity of one muscle may affect another (2, 3). With these findings it became evident that investigation of muscle recruitment patterns and neuromuscular efficiency in healthy individuals compared to patients with knee OA in simple closed chain exercises might lead to a better understanding of how knee OA develops (4). Although some studies have reported abnormal muscle activity in patients with OA, there are no studies that describe the modulation of this activity due to, for example, a change in velocity or distance of movement. change in time or distance (7) both in normal control and after OA. Comparison of average EMG and GFR in 4 inch (dotted) and 8 inch (line) Step Up/ Step Down task phases: Conclusion Step Down Task Step Up Task Step Up Task Vertical GRF References • Rana S. H, Bennel K. L., Metcalf B. R., Crossley K. M., 2002, “Delayed onset of Quadriceps activity and altered knee joint kinematics during stair stepping in individuals with knee Osteoarthritis” Arch Phys Med. Rehabilitation, 83, pp. 1080-1086. • Bhatia D., Bansal G, Joshi D., Anand S., Tewari R.P. 2011, “Coordination between lower limb muscles in different locomotion activities”International Journal of Biomedical Engineering and Technology, 6 (2), pp. 23-30. • De Luca, C.J. 1997, ‘The use of surface electromyography in biomechanics’, Journal of Applied Biomechanics, 13 (2), pp.135–163. • Childs J.D., Sparto P.J., Fitzgerald G.K., Bizzzini M., Irrgang J.J., 2004 “Alterations in lower extremity movement and muscle activation patterns in individuals with knee osteoarthritis” Elsevier Science Direct Clinical Biomechanics, 19, pp. 44-49. • Likivainio T. and Arokoski J.P.A, 2008 “Physical function and properties of Quadriceps femoris muscle in men with knee Osteoarthritis” Arch Phys Med Rehabil, 89, pp. 2185-2193. • Rana S. H., Hunt M.A., Creaby M.A., Wrigley T.A., McManus F.J., and Bennell K.L., 2010 “Hip Muscle Weakness in Individuals with Medial Knee Osteoarthritis” Arthritis Care & Research, 62 (8), pp. 1190-1193. • Pai Y.C., Chang H.J., Sinacore J.M., Lewis J.L., 1994 “Alteration in multijoint dynamics in patients with bilateral knee osteoarthritis”, Arthritis Rheum. Sep., 37 (9), pp.1297-304. Methods Methods Step Down Task • Three trials per subject were recorded employing dual AMTI force plates for measuring the GRF and EMG was measured using an 8 channel Motion Lab Corp. system, with both systems sampled at 1000 Hz (2nd order Butterworth filter with 20-500Hz cutoff). • The subject stepped from one force plate to another with the stance leg being stationary. The recorded EMG data was averaged across these trials for each subject; full wave rectified and analyzed employing EMG signal processing techniques (3). The GRF data was used to identify the different phases of movement and matched with the subsequent EMG data in Visual 3D software. Acknowledgement • I would like to thank the ANS Lab for allowing me to be a part of this team and gain an insightful experience that I know will benefit me in my future. I would also like to thank Dr. Dinesh Bhatia and Dr. Ranu Jung who have been very supportive throughout the research. Lastly, I would like to thank Dr. Denis Brunt and the Physical Therapy Department, FIU for providing support during data collection in the human performance lab and guidance during the research. Figure 2: Comparison of EMG patterns (average trials of one subject) in different 4 inch (dotted) and 8 inch (solid) Step Down task phases: 1. Initiation of movement, 2. Take off, 3. Landing, 4.Loading response, 5. Stabilization Contact Leg step down (Z) GRF EMG VastusLateralis, (maximum between 1-2) EMG Gluteus Medius, (maximum between 2-3) EMG Gluteus Maximus, (maximum between 3-4) Figure 1: Comparison of 4 inch (dotted) and 8 inch (solid) Step Up task phases: 1. Initiation of movement, 2. Toe- off, 3. Contact, 4.Stability Stability Leg (Z) GRF Stability Leg (X) GRF EMG VastusLateralis EMG Biceps Femoris EMG Gluteus Maximus