Transplantation
Transplantation. Xiang Li, Urology Department West China Hospital, Sichuan University. Acknowlegement. To Dr. Lu Yiping and Dr. Wang jia To other Colleagues working on renal and liver transplantation. Transplantation is a Dream?. Dream of Paranoia

Transplantation
E N D
Presentation Transcript
Transplantation Xiang Li, Urology Department West China Hospital, Sichuan University
Acknowlegement To Dr. Lu Yiping and Dr. Wang jia To other Colleagues working on renal and liver transplantation
Transplantation is a Dream? • Dream of Paranoia • Dream of excellent surgeon who wants to excel himself. • Dream of excellent scientist who believe nothing is impossible.
Can you imagine? Can you imagine? Can you imagine?
Contents • Basic concepts of transplantation • Clinical Organ transplantation • Renal Transplantation, RT • Transplantation Immunology • MHC and Tissue Matching • Graft Rejection • Immunosuppression
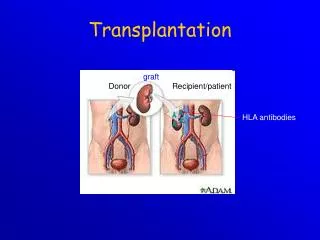
Definition of Transplantation • Implantation of „non-self” tissue into the body • the process of taking cells, tissues, or organs called a graft (transplant), from one part or individual and placing them into another (usually different individual). • donor: the individual who provides the graft. • recipient or host: the individual who receives the graft.
Blood Transfusion • First attempts were unsuccesful (MISMATCH) • Discovery of blood groups (Red cell antigens) • A-B Landsteiner 1900 • Rh Levine, Stetson 1939 • Succesful transfusion = Transplantation • Others: Bone, Tissue-engineering, etc • Transplantation • Organ Transplantation
Classification of Renal Transplantation • Auto-RT Cadaveric • Allograft RTLiving related Living Donor Living unrelated • Xenograft RT (In experimental)
Transplantation History • experimental kidney transplantation -1912 • Alexis Carel-Nobel prize • 1935 human kidney transplant in Russia - rejection • P.B. Medawar (1945) skin grafts • Self skin accepted • Relative not accepted ! What is the difference ? • Immunologic mechanism • A. Mitchison (1950) • Lymphocytes are responsible for rejection
Transplantation History • Peter Gorer (~1935) • Identification of 4 group of genes for RBC • Gorer and Gorge Snell (~1950) • Group II antigens are responsible for rejection • Major HistoCompatibility genes (HLA) • Nobel prize 1980 George Snell • 1954 Succesful kidney transplant between identical twins in Boston – Peter Bent Brigham Hospital • Joseph Murray 1991 Nobel prize
HISTORY OF THE RT • 1933 First clinical RT (Voronov); • 1954 First long-term successful RT(Twin); • 1958 Discovery of HLA(Human Lym Antigen); • 1959 Radiation be used for immunosupp- ression; • 1961 Azathioprine (Aza); • 1962 Prednisolone; Tissue Matching; • 1966 Cross-Matching; • Late 1960’ Preservation the Kidney>24hr ; • 1972 First successful RT(LRD) in china; • 1978 Clinical use of Cyclosporine(CsA).
Key factors for succesful transplantation • Knowledge of MHC haplotypes • Effective immunosuppression • Ability to identify and treat infections • Available donors
Clinical Organ Transplantation Liver Transplantation Renal Transplantation
LIVER TRANSPLANTATION • Indication: End stage liver diseases (ESLD) • Hepatic Disease to ESLD • Congenital malfomation; • Congenital liver metabolic disorders; • Acute liver failure; • Chronic liver failure: (1) Cirrhosis: Hepatitis B, Alcoholic; (2) Parasites: Hydatid disease of liver, ect. • liver malignance
RENAL TRANSPLANTATION END STAGE RENAL DISEASES (ESRD) Definition: (1) Various causes; (2) Irreversible injury; (3) Functional failure. Morbidity • Europe:50/million; • China:90-100/million
TREATMENT OF ESRD • DIALYSIS Chronic Ambulatory Peritoneal Dialysis (CAPD); Hemodialysis (HD). • KIDNEY TRANSPLANTATION
Renal Transplantation • Renal transplantation is associated with as survival benefit for patients with ESRD when compared to dialysis; • Even marginal donor kidneys confer a significant survival advantage over maintenance dialysis. • The preferred therapy for most of the Pts with ESRD; • More cost- effective; Better survival; Better life quality.
CONTRAINDICATION • Active invasive infection; • Active malignance; • High probability of operative mortality; • Unsuitable anatomic situation for technical success; • Severe psychological or financial problem.
Pre-OP Selection • ABO Blood Group:Compatible; • Cytotoxicity Test: Donor Lymphocyte Recipient Serum • Cross matching Donor Lymphocyte Recipient Serum Donor Serum Recipient’s Lymphocyte • Mixed Lymphocyte Culture • Tissue typing (HLA)
OPERATION DONOR (1)Living donor • Nephrectomy via flank approach; • Nephrectomy via Laparoscope.
(2) Cadaveric Donor • Total midline incision; • in situ flashing: Euro-collins/UW solution; • Bilateral radical nephrectomy. • Low temperature preservation.
Potential Advantages of living versus cadaveric kidney donor • Better short-term result(about 95% versus 90 % 1-yr function); • Better long-term results(half-life of 12-20 yr versus 8-9 yr); • More consistent early function and easy of management;
Potential Advantages of living versus cadaveric kidney donor • Avoidance of brain death stress; • Minimal incidence of delayed graft function; • Avoidance of long wait for cadaveric transplant;
Potential Advantages of living versus cadaveric kidney donor • Capacity of time transplantation for medical and personal convenience; • Immunosuppressive regime may be less aggressive; • Help relieve stress on national cadaver donor supply; • Emotional gain to donor.
Potential disadvantages of live donation • Psychological stress to donor and family; • Inconvenience and risk of evaluation process(i.e., intravenous contrast); • Operative mortality(about 1 in 2000 Pts.); • Major post operative complications (about 2% of Pts.);
Potential disadvantages of live donation • Minor postoperative complications(up to 50% of Pts.); • Long-term morbidity(possible mild hyper-tention and proteinuria); • Risk for traumatic injury to remaining kidney; • Risk for unrecognized covert chronic renal disease.
Recipient Operation Extraperitoneally in the contralateral iliac fossa via Gibson incision. Why contralateral ?
RECIPIENT OPERATION • Blood Vessel Anastomosis: • Donor renal V Recipient’sexternal iliac V • Donor renal A Recipient’s internal iliac A • Ureter Anastomosis: • Donor ureter Recipient’s bladder • Anti-reflux anastomosis
Clinical phases of rejection • Hyperacute rejection(minutes to hours) • Preexisting antibodies to donor HLA antigens • Complement activation, macrophages • Accelerated rejection • Acute rejection(around 10 days to 30 days) • Cellular mechanism (CD4, CD8, NK, Macrophages) • Chronic rejection(months to years !!) • Mixed humoral and cellular mechanism • CHRONIC REJECTION IS STILL HARD TO MANAGE !
IMMUNOSUPPRESSION • Immunosuppresents play a very impor-tant role in organ transplantation; • Immuosuppresents extremely increase the effect and the survival rate of organ transplantation;
IMMUNOSUPPRESSION • Immunosuppresents are a double - edged sword; • the most important thing is to increase their positive effects, and in the same time decrease their side effects (i.e., organ toxicity, infection, tumors, ect.).
Diagnosis of rejection Symptom/Sign • fever; • urinary output ; • graft tenderness; • graft size ; • hypertension; • myalgia/arthragia.
Laboratory Test • Serum creatine, SCr; • Urinary creatine, Ucr; • Color doppler scan; • radiorenogram; • Ateriogram; • Biopsy: (1) Fine needle aspiration biopsy (FNAB); (2) Core needle biopsy(CNB).
Treatment of kidney rejection • Hyperacute (Sometimes during the operation !) • No therapy, usually results in graft failure – kidney should be removed • Acute (Most frequently in the first 4 weeks) • BIOPSY ! • Increase immunosuppression • Increase steroid dose • Increase cyclosporin (monitor serum level !) • ATG, ALG, OKT3 • Chronic • ACE inhibitors, prostacyclin analog drugs • Steroid, Imuran, Cellcept
Histocompatibility Antigens • Major histocompatibility antigens • MHC class I molecules : almost all nucleated cells • MHC class II molecules : APCs, endothelium of renal arteries and glomeruli • Minor histocompatibility antigens : H-Y molecule