Antidiabetic Drugs
Antidiabetic Drugs. Criteria for Diagnosis of DM DM Screening. Symptoms of diabetes + casual plasma glucose level less than or equal to 200 mg/ dL OR Fasting plasma glucose higher than or equal to 126 mg/ dL OR


Antidiabetic Drugs
E N D
Presentation Transcript
Criteria for Diagnosis of DMDM Screening • Symptoms of diabetes + casual plasma glucose level less than or equal to 200 mg/dL OR • Fasting plasma glucose higher than or equal to 126 mg/dL OR • 2-hour postload glucose level higher than or equal to 200 mg/dL during an oral glucose tolerance test • Impaired glucose tolerance (IGT) • FPG <110 mg/dL: normal fasting glucose • FPG ≥110 mg/dL but <126 mg/dL: impaired fasting glucose (IFG) • FPG ≥126 mg/dL: provisional diagnosis of diabetes mellitus
Optimal Levels of Blood Sugars • Preprandial-110 mg/dl • Postprandial-180 mg/dl
Diabetes Mellitus Facts • Of the 16 million Americans – 5 million are probably unaware they • 2,000 per day are diagnosed with DM • Causes 200,000 deaths annually • 6th leading cause of death • Leading cause of blindness • Causes >50% of nontraumatic lower-limb amputations • Leading cause of end stage renal disease
Diabetes Mellitus • Two types • Type 1 • Type 2
Type 1 Diabetes Mellitus • Lack of insulin production OR • Production of defective insulin • Affected patients need exogenous insulin • Complications • Diabetic ketoacidosis (DKA) • Hyperosmolar nonketotic syndrome • Oral antidiabetic drugs not effective
Diabetes Mellitus • Symptoms • Polyuria • Polydipsia • Polyphagia • Glycosuria • Unexplained weight loss • Fatigue • Hyperglycemia
Type 2 Diabetes Mellitus • Most common type • Caused by insulin deficiency and insulin resistance • Many tissues are resistant to insulin • Reduced number insulin receptors • Insulin receptors less responsive
Type 2 Diabetes Mellitus • Several comorbid conditions • metabolic syndrome OR insulin-resistance syndrome OR syndrome X • Obesity • Coronary artery disease • Dyslipidemia • Hypertension • Microalbuminemia (protein in the urine) • Enhanced conditions for embolic events (blood clots) • Insulin Resistance
Treatment DIfferences • Type 1 • Exogenous insulin • Dietary control • Type 2 • Lifestyle changes • Dietary control • Weight reduction • Exercise • May require oral hypoglycemic therapy or exogenous insulin • Insulin when oral hypoglycemic medications can no longer provide glycemic control
Gestational Diabetes • Hyperglycemia that develops during pregnancy • Insulin must be given to prevent birth defects • 4% of all pregnancies • Must be reclassified if it persists 6 weeks post-delivery • Usually subsides after delivery • 30% of patients may develop Type 2 DM within 10 to 15 years
Hyperglycemia Blood Glucose >110 Insulin Resistance Decreased Insulin Increased Free Fatty Acid Oxidative Stress
Oxidative Stress Nitric Oxide Nitric oxide Tissue factor Plasminogen Activator Prostaccyclin Nitric Oxide Angiotensinll Endothelin-1 Activation of activator protein -l Angiotensinll Vasoconstriction Inflammation Thrombosis hypertension Release of chemokines Release of cytokines Expression of cellular adhesion molecules Vascular smooth muscle cell growth Hyper coagulation Platelet Activation Decreased Fibrinolysis
Major Long-Term Complications of DM (Both Types) • Macrovascular (atherosclerotic plaque) • Coronary arteries • Cerebral arteries • Renal arteries • Peripheral vessels • Microvascular (capillary damage) • Retinopathy • Neuropathy • Nephropathy
Macrovascular (atherosclerotic plaque) • MI • DVT • PE • Stroke • AAA • Retinopathy
Hyperglycemia Metabolic Stress Response Stress hormones and peptides Increased Glucose Decreased Insulin
Increased Glucose Decreased Insulin Increase in: Ketones Free Fatty Acids Lactate Immune Dysfunction Reactive 02 Species Cellular Injury Inflammation Tissue Damage Altered Tissue Healing Acidosis Thrombosis Global Infarction Ischemia Infection Dissemination Increase Transcription Factors Leads to Secondary Mediators
Complications Associated with Diabetes Mellitus • Cardiovascular disease, including hypertension • Peripheral vascular disease • Delayed healing • Visual defects, including blindness • Renal disease • Infection • Neuropathies • Impotence
Types of Antidiabetic Drugs • Insulins • Oral hypoglycemic drugs Both aim to produce normal blood glucose states
Insulins • Substitute for & same effects as endogenous insulin • Restores the diabetic patient’s ability to: • Metabolize carbohydrates, fats, and proteins • Store glucose in the liver • Convert glycogen to fat stores • Some derived from porcine sources • Most now human-derived, using recombinant DNA technologies • Goal: tight glucose control • To reduce the incidence of long-term complications
Human-Based Insulins • Rapid-Acting • Most rapid onset of action • Shorter duration May be given SC or via continuous SC infusionpump (but not IV)
Human-Based Insulins • Short-Acting • regular insulin (Humulin R, Novolin R) • Onset 30 – 60 minutes • The only insulin product that can be given by IV bolus, IV infusion, or even IM
Sliding-Scale Insulin Dosing • SC rapid or short-acting doses adjusted according to blood glucose test results • Typically used in hospitalized diabetic patients • Or in patients on TPN / enteral tube feedings or receiving steroids • Subcutaneous insulin is ordered in an amount that increases as the blood glucose increases
Human-Based Insulins • Intermediate-Acting • isophane insulin suspension (also called NPH) (Humulin N, Novolin N) • isophane insulin suspension & insulin injection (Humulin 50/50 , Humulin 70/30, Novolin 70-30) • Lispro protamine suspension (Humalog 75/25, Novolog Mix 70/30) • insulin zinc suspension (Lente, Novolin L) • Cloudy appearance • Slower in onset and more prolonged duration • than endogenous insulin
Human-Based Insulins • Combination Insulin Products • NPH 70% and regular insulin 30% (Humulin 70/30, Novolin 70/30) • NPH 50% and regular insulin 50% (Humulin 50/50) • insulin lispro protamine suspension 75% and insulin lispro 25% (Humalog Mix 75/25)
HbA1c • It is a test that allows healthcare providers to see how diabetics have managed their blood glucose level over the last 2-3 months….
Insulin • Storage: • Neither be allowed to freeze or heated above 98oF • Store in refrigerator until opened • Once opened, store at room temp: 68o to 75oF • Once opened, discard after 30 days • Avoid excess agitation – gently roll in the palms of hands (not shaken) to warm and resuspend insulin
Insulin Injection SitesLipodystrophies • Atrophy or hypertrophy • Dermatologic conditions • Hypertrophy more common • Fat pads become anesthetized • Results in prolonged & erratic insulin absorption • Loss of diabetic control
Oral Antidiabetic Drugs • Used for type 2 diabetes • Treatment for type 2 diabetes includes lifestyle modifications • Diet, exercise, smoking cessation, weight loss • Oral antidiabetic drugs may not be effective unless the patient also makes behavioral or lifestyle changes
DM MonitoringGlycosylated Hemoglobin Assays • HbA1c • Good indicator of the average blood glucose levels. • Shows the average blood glucose level during the previous 120 days • Used to assess long term glycemic control • Performed at diagnosis and at specific intervals to evaluate the treatment plan • Altered by pregnancy, increased triglycerides & bilirubin • Twice annually for patients with good control • Quarterly for patients whose therapy has changed
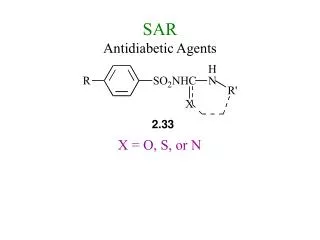
Oral Antidiabetic DrugsSulfonylureas • First generation: • chlorpropamide (Diabinese), • tolazamide (Tolinase) • tolbutamide (Orinase) • Second generation: • glimepiride (Amaryl) • glipizide (Glucotrol) • glyburide (DiaBeta, Micronase)
Oral Antidiabetic Drugs:Sulfonylureas Sulfonylureas • Stimulate insulin secretion from the beta cells of the pancreas, thus increasing insulin levels • Beta cell function must be present • Improve sensitivity to insulin in tissues • Result: lower blood glucose levels • First-generation drugs not used as frequently now
Oral Antidiabetic Drugs: Sulfonylureas --Adverse Effects • Sulfonylureas • Hypoglycemia • hematologic effects • nausea • epigastric fullness • heartburn • many others