Download
1 / 62
620 likes | 855 Vues
Bronchiectasis Questions. Dean E. Schraufnagel, MD ATS President-Elect University of Illinois at Chicago May 6, 2010 Nothing to disclose. ATS Founder. American Thoracic Society: An International Society.

E N D
Bronchiectasis Questions Dean E. Schraufnagel, MD ATS President-Elect University of Illinois at Chicago May 6, 2010 Nothing to disclose
ATS Founder
American Thoracic Society: An International Society • ATS International Conference (May 14-19, 2010 New Orleans) features over 5,500 original research presentations with 16,000 attendees • About half of participants from outside the US • American Journal of Respiratory and Critical Care Medicine has the highest impact factor in respiratory or critical care medicine • Over half of articles submitted to ATS journals come from outside the US
We know about Bronchiectasis … or do we?
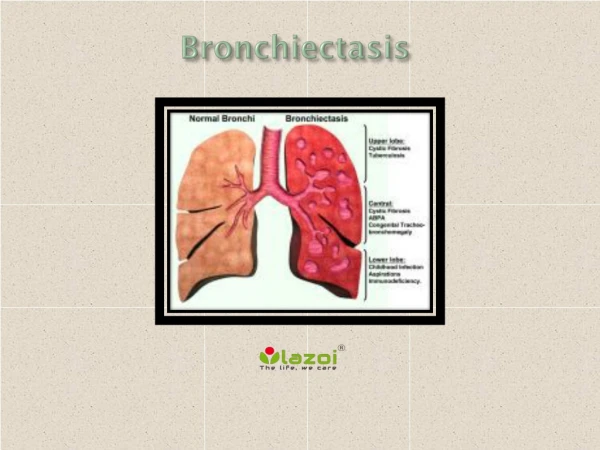
Definitions • “Permanently” dilated bronchi Reid. Thorax 1950;5:233-47 • 1.5 x larger than accompanying artery Desai et al., Br J Radiol 1994;67:257-62 • Larger than accompanying artery Li et al., Eur Resp J 2005;26:8-14 • What about • Bronchial wall thickness? • Tree in bud? • Reversible?
Is bronchiectasis in different locations different Diseases?
Commonly held • Upper lobe – TB • Middle lobe – environmental mycobacteria • Lower lobe – post-infectious • Central – allergic aspergillosis • Focal – obstruction • Diffuse – agammaglobulinemia
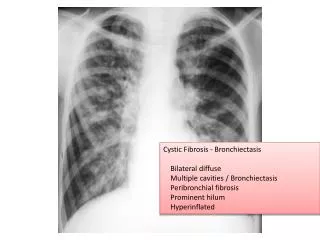
Upper lobe → tuberculosis • Old or active tuberculosis • Unsuspected until hemoptysis • Other upper lobe • Cystic fibrosis • Sarcoidosis • “Dry bronchiectasis” • Post-TB, Sjögren's, unable to expectorate • Yazisiz et al., Rheumatol Int. 2009
Mother had TB. Skin test positive
Middle lobe • Middle to older-aged, nonsmoking ♀ • Mitral valve prolapse & chest deformity • Why environmental mycobacteria? • Why middle lobes? • Clearance?
Allergic bronchopulmonary aspergillosis • Eosinophilia, transient alveolar opacities, ↑IgE (specific), precipitins, immediate skin test • Paradox • Intense inflammation - Rx steroids • But oral steroids ∝ poor outcome • Itraconazole
Lower-lobe How often is it not associated with an etiological Infection?
Focal – Obstruction? • Bronchoscopy? • Other focal areas often present • Important if considering surgery • Gursoy et al., Surgery Today 2010;40:26-30
Diffuse - Immune deficiency? • Immune deficiency • Common variable, HIV • Global airway disease • Mounier Kuhn, papillomatosis, relapsing polychondritis • Advanced bronchiectasis of any type
♀ - cc: cough and breathlessness (on questioning-hemoptysis) → Interstitial lung disease → Biopsy
Pathogenesis • Secretions not cleared • Organisms grow in secretions • Immune response → ongoing inflammation • Hyperemia, vascular hyperplasia • Bronchospasm • Peribronchial tissue destruction • Upper lobe→ less secretions, less destruction?
Pathogenesis • Organisms remain external to body • Reason for mild symptoms? • Difficulty in treating and diagnosis • Immune cells - less impact • Antibiotics - less penetrance • Little abscesses? • Organisms protected by secretions? • Reason for inadequate treatment?
Excess matrix metalloproteinases • Breakdown tissue • 1607GG allele of promoter MMP1 • ↑ 37 bronchiectasis pts cf 102 nl • Heterozygote O.R. = 5.3 • Homozygotes O.R. = 8.7 • Stankovic et al., J Investig Med 2009;57:500-3
Lung PMN dysfunctional? • Bronchiectatic sputum: ↑ Human neutrophil peptides • ∝Defective phagocytosis • Multiple PMN ∆’s controlled by i.c. Ca2+ • Also found in α1-antitrypsin animal model • Voglis et al., Am J Respir Crit Care Med 2009;180:159-66 • Low neutrophil oxidative burst • IFNγ restores • King et al., APMIS 2009;117:133-39
What about biofilms?
Biofilms • Complicated slime layers • Glycoprotein matrix from bacteria • E.g. dental plaque • Acinetobacter & pseudomonas – more stable than ancestral colonies • Hansen et al., Nature 2007;445:533-6 • M. mucogenicum & B. cepacia→↑biofilm • Simões et al., Appl Environ Microbiol 2007;73:6193-6200
Complex communities • Antagonistic, competitive, commensal, or symbiotic • Benefits • Plasmid sharing • Metabolism sharing • Defense sharing • Disadvantage – nutrient competition • Biofilm mass ↯∝ metabolic activity Simões et al., Appl Environ Microbiol 2007;73:6193-6200
Biofilms Protect inhabitants
Biofilms protect inhabitants • Macrophage engulfment ↓ • Antibiotic penetration ↓ • ↑antibiotic resistance • ↓ stimulation to mucosa • Bacteria switch to latent form • pH, nutrient Δ • Exacerbation - bacteria emerge from biofilm?
Quorum sensing • Bacteria ↦molecules ∝ population density • E.g. Gram neg: Acylated homoserine lactones • Sensing → Δ gene expression • ↦ virulence factors, biofilm, antibiotic production, swarming, conjugation, sporulation, bioluminescence • Autoinducer
Treatment potential? • Quorum sensing inhibitors • ↛ gene regulation, production, reception • Enzymes inactivate QS molecules • ↛ biofilm • Fewer toxic effects? • Not required for bacterial growth • Animals and plants →↑survival • Rasmussen & Givskov. Microbiol 2006;152:895-904
Which organisms important? • Most common in established bronchiectasis • H. influenza (47%), P. aeruginosa (12%) • King et al., Resp Med 2007;101:1633-8 • Multiple species • Role of mouth flora? • Role of mycobacteria? • Role of in vitro antibiotic testing?
Low virulent organisms? Low virulence Little damage, invasiveness Living in biofilm different than culture? UIC BAL - stomatococcus ~15% Often “normal respiratory flora” How do deal with it? No growth - adequate sputum? Mycobacteria, fungi, handling problem