Managing Post-Traumatic Stroke Disorder: Cognitive Errors in Diagnosis
10 likes | 98 Vues
Learn about cognitive errors in diagnosing post-traumatic stroke disorder, common presentation characteristics, and the impact of misdiagnosis on patient outcomes. Case studies highlight key takeaways. References to medical malpractice and adverse events included.

Managing Post-Traumatic Stroke Disorder: Cognitive Errors in Diagnosis
E N D
Presentation Transcript
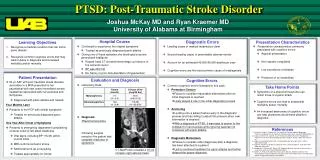
PTSD: Post-Traumatic Stroke Disorder Joshua McKay MD and Ryan Kraemer MD University of Alabama at Birmingham Diagnostic Errors Presentation Characteristics Learning Objectives Hospital Course • Continued to experience her original symptoms • Treated as previously diagnosed panic attacks • During one of these episodes she developed a severe generalized headache • Repeat head CT showed hemorrhagic conversion of the ischemic lesion • BP was 234/140 • No history or prior documentation of hypertension • Leading cause of medical malpractice claim • Second leading cause of preventable adverse events • Account for an estimated 40,000-80,000 deaths per year • Cognitive errors are the most common cause of misdiagnosis • Presentation characteristics commonly associated with cognitive errors: • Atypical presentation • Non-specific complaints • Low prevalence of disease • Presence of co-morbidities • Recognize a medical condition that can mimic panic attacks • Recognize common cognitive errors that may lead to delay in diagnosis and increased morbidity and/or mortality Patient Presentation Evaluation and Diagnosis Cognitive Errors • 54 yo AAF with post traumatic stress disorder secondary to a MVA presented to her psychiatrist with new onsetintermittent severe headaches associated with nervousness and tachypnea • Diagnosed with panic attacks and treated • Four Months Later • Presents to her PCP with similar symptoms • Treated for previously diagnosed panic attacks • One Year After Onset of Symptoms • Presents to emergency department complaining of acute onset of left-sided weakness • Vital signs, including BP 115/48, within normal limits • MRI confirms ischemic stroke • Additional work-up unrevealing • Treated appropriately for stroke • Laboratory Data: • Diagnosis: • Pheochromocytoma • Following surgical resection the patient had complete resolution of symptoms • Common cognitive errors illustrated in this case: • Premature Closure • Failure to consider reasonable alternatives after an initial diagnosis is reached • Likely played a role in the initial diagnostic process • Anchoring • Locking onto a salient feature early in the diagnostic process and then failing to adjust this process when new information is obtained • With a diagnosis of PTSD, it was easy to anchor to the complaint of nervousness while ignoring features not consistent with panic attacks • Diagnostic Momentum • Failure to consider other diagnoses after a diagnosis has been attached to a patient • Led to continued treatment for panic attacks and further delayed the proper diagnosis Take Home Points • Symptoms of a pheochromocytoma can mimic those of a panic attack • Cognitive errors can lead to substantial morbidity and/or mortality • An increased awareness of cognitive errors can help physicians avoid these pitfalls in diagnosis. References 1. Chandra A, Nundy S, Seabury SA. The Growth of Physician Medical Malpractice Payments: Evidence from the National Practitioner Data Bank. Health Aff 2005;W5240-9. 2. Leape LL, Brennan TA, Laird N, et al. The Nature of Adverse Events in Hospitalized Patients-Results of the Harvard Medical Practice Study II. N Engl J Med 1991;324:377-84. 3. Leape LL, Berwick DM, Bates DW. Counting deaths due to medical errors. JAMA 2002;288(19):2405. 4. Graber M, Franklin N, Gordon R. Diagnostic error in internal medicine. Arch Intern Med 2005;165:1493-1499. 5. Kostopoulou O, Delaney BC, Munro CW. Diagnostic difficulty and error in primary care - a systematic review. Fam Pract 2008;25(6):400-13. 6. Redman JC, Peloso OA, Milne RL, Kaminsky NI, Ellis SC, Wolfel DA, Martinez PU. Asymptomatic pheochromocytoma. Diagnosis after hemorrhagic stroke in a middle-aged patient. Postgrad Med 1983;73(4):279,282-5. CT-Abd/Pelvis revealed a 10 cm complex right adrenal mass