Download

1 / 31
360 likes | 728 Vues
Cleft palate … .questions to be answered?. There is no such thing as a stupid question . Socrates.

E N D
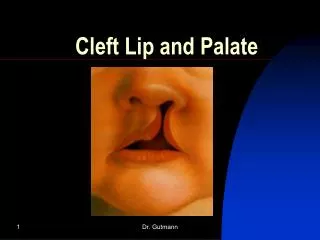
This brief description was written by a person with cleft palate to be born in sweden on December 6,1774. It outline the problems caused by the cleft of lip and palate: esthetic defect , difficulty in communication (nasalization), and inability to suck. Hail God. The great Creator! he has brought me to this Valley of Tears marked by a Deformity, which I bring on my body. on my face. for every body to see. But another defect lays unseen. in the roof of my mouth. which confounds my Speech. sadly. keeping me apart from other Men . Not being able to nurse. due to my deformity.
Q1-what is typical time for cleft palate repair? (Early repair affect growth, late repair affect the speech)! -Brophy and Veau first recognized the beneficial effect of early cleft palate closure on speech in early part of last century , but it was not until the 1940s where refinement in surgical procedures and anesthetic technique improved the safety of this procedure during the first year of life. -Graber report and other in 1940s and 1950s document significant maxillary growth restriction for early palatoplasty which lead to delayed repair to age of 5 and 6 years.
-current concept is to repaired cleft plate either single stage around age of 11-12 months OR two-stage repair with soft palate at time of lip repair and hard palate repaired before 18 months or delayed further. Is very early repair of palate(3-6) improved results in regarding to speech? Although there are some logical reasons for repairing the velum at 3-6 months of ages, there are few solid data to support this approach. certainly, the potential benefits of such early repair must be weighted against the risk of anesthesia and tolerance for blood loss and poor surgical exposure with all structure are small.
Q2:One- or Two-Stage Palate Repair? -Gillies and Fry first mentioned the idea of two-staged palate repair in response to poor maxillary growth(1921). -Schweckendieks have used this procedure with excellent facial growth outcome. the soft palate is repaired early to allow for normal speech, but hard palate closure is delayed until the age of 12 to 14 years(1939). -Zurich team and the Go¨teborg team have also used the 2two stage method successfully, with different time.(7 and 9 years respectively). however not every team found superior maxillary growth after delayed hard palate closure. There are reports suggest negative speech outcome in delayed hard palate repair.
-Chang Gung Craniofacial Center, Taipei, Taiwan between 1978 and 1982 They adopted protocol involved staged palate repair with closure of the soft palate at 1 year of age and the use of a removable speech prosthesis until closure of the hard palate at the age of 6 years. Follow up of patients by 2 parameters : cephalometric study and adequate velopharyngeal function.
From the results, concluded that in patients with unilateral cleft lip and palate, one-stage versus two-stage with delayed hard palate closure, has a significant adverse effect on the growth of the maxilla. Two-stage repair has a smaller adverse effect on the growth of the maxilla than one-stage repair. This stage effect is on the anteroposterior development of the maxilla and is attributable to the development being undisturbed before closure of the hard palate (i.e., hard palate repair timing specific). Stage of palate repair does not significantly affect the growth of the mandible. But worse speech outcome in term of more articulation error when the hard palate repair delayed to 4 years of age. It was abandoned in this center in 1982, this abandonment was based on philosophy that speech consideration should be the main determine in cleft palate surgery.
Q3:Is Nasal Mucoperiosteal Closure Necessary inCleft Palate Repair? the necessity of stripping the mucosa of the vomer and/or nasal side of the maxilla to establish nasal floor closure has not been studied or tested.
Advantages: -Single layer closure provided less operative time(84 mints in compares with 2 layers closure 135 minutes) and enhanced simplification of the operation. • -In one study show no significant increased risk of fistula formation ,which mean that nasal layer repair not decrease incidence of fistula formation in palatal repair. -Decreased the restrictive effect on maxillary growth
Q4:Does Palatal Muscle Reconstruction Affect the functional outcome of cleft palate?:The objective of cleft palate surgery 1-close the palate to restore normal function to eating and drinking. 2-enhance the development of normal speech. 3-eustachian tube aeration of middle ear. 4-normal facial growth
In cleft palate the muscle is hypoplastic and attach to posterior margin of hard palate rather than midline raphe
-Victor Veau actually first advocated midline levator palatini reapproximation. -Cutting has described a technique of veloplasty that include division of tensor palatini tendon and repositioning of muscle at hamulus.
-A controlled, prospective study conducted by Marsh et al found no difference between intravelar veloplasty and traditional side to side technique on VPI. -Sommerlad has adopted a technique for radical retropositioning of the velar musculature and tensor tenotomy using an operating microscope, His experience with this technique resulted in a significant decrease in secondary velopharyngeal rates for successive 5-year periods from 10.2% to 4.9% to 4.6%. -In a prospective cohort study conducted by Hassan et al, a comparison of three layer palatoplasty (Kriens technique) with intravelar veloplasty versus two-layer palatoplasty (Wardill- Kilner) pushback palatoplasty without intravelar veloplasty has shown that palatal muscle reconstruction in cleft patients offers better velopharyngeal competence and eustachian tube function
-Kriens palatoplasty involves modification of Wardill-kilner V-Y pushback technique, in which submucosal dissection of muscle on the nasal side and then reconstruction of the palatal muscle in the midline and three layer closure are performed. Palatal muscle reconstruction in cleft palate patients confers better functional results regarding velopharyngeal competence and Eustachian tube function.
Q5:wide cleft palate…solutions? -Surgical repair of wide cleft palate has been proven formidable task to the surgeon. Wide cleft palate define as bony palatal shelf less than one third the width of cleft defect.
Solutions: 1-many of these patients are adequately managed by use prosthetic speech appliance design to occlude the defect and obtain velopharyngeal competence.
2- A number of technique have been described for lengthening of the pedicle including ostotomies of foramen so get tension free closure. 3-tubed skin flap have been used, but staged procedure and poor speech result and halitosis was encounter.
4-To ensure tension free closure for a wide cleft palate, immediate placement of a posterior pharyngeal flap during primary palatoplasty. -Bengt Johanson first described an elongated pharyngeal flap for extremely wide cleft palate closure. A primary pharyngeal flap with a two-flap palatoplasty is often required to close un-repaired cleft palates in adults as it is frequently associated with palatal tissue hypoplasia and a wide cleft.
5- soft tissues expansion: Two types of expansion regimens are used clinically: conventional, prolonged expansion for 1–3 months and intraoperative tissue expansion called ‘‘intraoperative sus- tained limited expansion’’ Self-expanding expanders manufactured by OSMED(Ilmenau, Germany) were implanted under the mucoperiosteal layer of the hard palate, on purpose to generate more tissue and provide facility for palate repair performed 24–48h later
8-The use of buccal fat pad (BFP) as a pedicled graft in cleft palate surgery
Q6:posterior pharyngeal flap or sphincter pharyngoplasty for treatment VPI? Pattern of VP closure: 1- Coronal (55%) 2- Circular(20%) 3- Circular with Passavant ridge(15%) 4- Saggital(10%)
-Pensler and Reich retrospective compared 75 patients with VPD treated by pharyngeal flap to 10 patients treated by sphincter pharynoplasty , noting no different in speech outcome. -Witt et al. examined velopharyngeal function in 65 patients after pharyngeal flap surgery and in 123 patients after sphincter pharyngoplasty. Persistent VPD requiring surgical revision was present in 20% of pharyngeal flap patients and 16% of sphincter pharyngoplasty patients. there appears to be an inverse relationship in most patients between postoperative symptoms of upper airway obstruction and residual VPD, suggesting that velopharyngeal competence may occasionally come at the cost of airway obstruction usually transient, particularly in patients undergoing pharyngeal flap procedures.
Q7:superior based or inferior based posterior pharyngeal flap? Indication of superior based pharyngeal flap: 1- if radiographic examination show maximum lateral pharyngeal motion to be high rather low. 2- If the space to be bridge is great. 3- If the palate need to be lengthening at same operation.
Indications of inferiorly based pharyngeal flap: 1- if the exposure is diffecuilt. 2- the pateint is in poor condition. 3- the palate is mobile that no need to do throough and through incision in soft palate.
Advantage of inferior based pharyngeal flap: 1- Act as sound board to direct air stream into mouth. 2- May located at level of greater amount of lateral pharyngeal motion. 3- it reconstruction not required opening the soft palate. 2- Lend itself well to secondary revision. - Skoog, Hamlen, whitaker believe that the position of the base of the flap made no different in long term outcome and make no different in length of hospital stay, complication, speech outcome, hearing result.