Download
1 / 36
360 likes | 470 Vues
This study investigates the relationship between the CCR2 V64I genetic variant and cardiovascular events in a diverse Dutch cohort. We explore the implications of the variant on major adverse cardiovascular events (MACE) and its role in atherosclerosis. Utilizing the Framingham risk score, we assess whether the CCR2 genotype modifies the risk of cardiovascular outcomes. The research contributes to understanding the genetic basis of atherosclerotic disease through extensive cohort data, including genetic and epidemiological analyses.

E N D
CCR2 variant and cardiovascular outcome in a general population-based cohort Mike Zuurman, PhD Internal Medicine/Nephrology UMCG, Groningen The Netherlands Breedtestrategie
Breedtestrategie Complex Trait analysis in man: Genetic basis of atherosclerotic end-organ damage
Clinical nephrology Clinical cardiology Functional nephrology Endocrinology Epidemiology Molecular biology Genetics Genomics Breedtestrategie Interdisciplinary strategy
Breedtestrategie • Three post-doc positions: • Genetic Epidemiology • Genetic molecular biology • Bioinformatics Project duration: 4 years
Genetic basis of atherosclerotic organ damage: From animal genetics to human cohorts QTL analysis / Mutagenesis atherosclerosis renal damage HDL cholesterol PLTP activity candidate genes functional studies functional studies Human populations
Advantages of QTL analysis QTL analysis allows identification of novel genes involved in the phenotype. QTL mapping is more likely to find mutations in rate limiting or regulatory genes, which will be very important therapeutic targets.
F F P P Complex Traits Diagram P + + P = trait = intermediate phenotype 9 Environment P 6 1 P EF 3 EF 5 2 G EF P EF 7 4 G G 10 Individual 1. env. response to phenotype (treatment), 2. env. influence on gene expression, 3. env. inducing internal phenotype, 4. env. influencing expression of unknown gene, 5. phenotypes combine to one detectable phenotype, 6. phenotype is only partly surfacing, 7. internal feedback mechanisms 8. unidentified gene influencing detectable phenotype, 9. un- visible/detectable/known phenotype 10. gene-phenotype-phenotype-gene interaction
Research Flow Genetic determinants of Atherosclerotic (End-Stage) disease in man • Functional analyses • In vitro/In vivo • Molecular • Fundamental • Genetic epidemiology • Patient cohorts • General population • Sequence variants Bioinformastatistica -Utilization of tools -Development of tools -Solutions
Genetical epidemiology • Cohorts • - PREVEND (8592/40000) • - NECOSAD (1000) • - Zwolle Diabetes (1200) • a.o. • Sequence variants • Single nucleotide polymorphisms • Haplotypes • Tandem repeats • Insertion/deletion • Cross sectional/prospective • Major adverse cardiovascular events • Microalbuminuria • Renal dysfunction
Genetical epidemiology • Cohorts • - PREVEND (8592/40000) • Sequence variants • Single nucleotide polymorphisms • Cross sectional/prospective • Major adverse cardiovascular events
Age Confounders • associated with exposure • related to the outcome • -not part of the causal pathway • Mother highly educated Child Down syndrome • Alcohol intake Lung cancer • Blood pressure UAE Smoking Gender
PREVEND design n=85.421 invited for pre-screening n=40.856 responded (47.8%) UAC < 10 mg/L n= 30.890 UAC >= 10 mg/L n= 9.966 Exclusion -pregnancy -insuline use -No informed consent n= 3.395 invited for screening 1 n= 2.592 responded (76.3%) n= 7.768 invited for screening 1 n= 6.000 responded (77.2%) n= 8.592 screening 1 1997-98
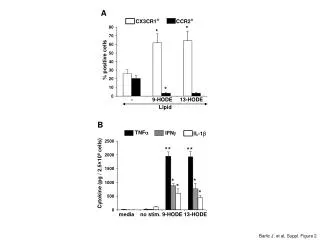
CCR2 About Basic • Ligand: CCL2 (MCP-1) • Gi-protein coupled • - Inhibits cAMP • Seven-transmembrane spanning • Hetero/Homo di- and multimers • Two splice variants (A and B) Functional • Intracellular calcium • Cellular migration (chemotaxis) • Pro-inflammatory • Atherogenesis • Angiogenesis
CCR2 p. V64I: a single nucleotide polymorphism (SNP) Nakayama et al.,AIDS 2004 Mar 26;18(5):729-38. Gives rise to a valine to isoleucine substitution
CCR2 p. V64I and cardiovascular outcome • 64I is associated with reduced coronary artery calcification • 64I is associated with higher prevalence of myocardial infarction CCR2 p. V64I and receptor function • Nakayama et al.(2004): CCR2A not CCR2B is altered • Increased surface expression of CCR2A • More stable expression of CCR2A • Increased down-regulation of CCR5
Research question Is risk of cardiovascular events modified by CCR2 V64I genotype? • Framingham risk score • Calculated using: • Sex • Age categories • Total cholesterol levels • HDL levels • Smoking status • (Treated) Systolic blood pressure • Indicates: • 10-year risk assessment for CHD/CVD • Atherosclerotic risk
PREVEND CCR2-V64I encoding allele frequencies • Population : • Caucasian • No missing genotype ∑ χ2: cumulative chi-square value for all genotypes (VV, VI and II).
MACE: Framingham risk range by CCR2 SNP 7 II + IV VV 6 5 4 O/E MACE 3 2 1 0 0-10 10-20 20-30 30+ Framingham Risk range Multivariate model : P = 0.008 for interaction genotype and FRR
CCR2 p. V64I and Framingham high risk (>30%) 40 VV VI + II 30 % MACE 20 10 0 No Yes Framingham high risk
MACE: Framingham SBP score by CCR2 SNP 30 VI+II (Men) VV (Men) 25 VI+II (Women) VV (Women) 20 % MACE 15 10 5 0 0 1 2 3 4 5 6 Framingham SBP score
History of antihypertensive treatment by CCR2 p. V64I P=0.004 * 30 VV II+IV 20 % 10 0 Non-hypertensives Hypertensives Prevalence of cardiovascular events during follow-up. CCR264I I-carriers show more cardiovascular events (P=0.004) than VV homozygotes in subjects with a history of antihypertensive Treatment. No difference was observed in non-hypertensives
Subjects on AHT drugs by CCR2 p. V64I No differences
Conclusions • CCR2 p. V64I modifies risk associated prevalence of MACE • in the general population, independantly of other confounders • The association is only apparent in high risk subjects • - Framingham Risk Score >10 % • - Hypertensive patients (treated) General idea The (biological) effects of SNPs or other gene variants on disease are likely to surface to detectable range only under conditions of advanced progressive pathology (i.e. when compensation no longer suffices).
Baseline characteristics and risk factors for mortality according to CCR2-V64I genotype
All-cause mortality hazard ratios of CCR2 VI subjects using Cox regression models and CCR2V64I VV-individuals as reference.
Conclusions: 1. CCR2 p. V64I associates with CV-events when subjects already suffer from hypertension 2. CCR2 p. V64I associates with all-cause mortality
Chemokines in pathology: renal disease J Am Soc Nephrol 11: 152-176, 2000
CCR2A / CCR2B in human renal tissue Acute rejection CCR2A CCR2B
CCR2A / CCR2B in human renal tissue Atherosclerotic vessel CCR2B CCR2A
Future research • Investigation of aortic/vascular sections • Differential expression of CCR2A/2B • Localisation by double staining • QPCR of fresh tissue -Possible association of CCR2 p. V64I with restenosis in CV patient cohort -In vitro study of effect of CCR2 p. V64I polymorphism on vascular smooth muscle cells
Department of Internal Medicine Subsection Nephrology Mike Zuurman Gerjan Navis Paul de Jong Trial Coordination Centre Hans Hillege Cardiology / Clinical Pharmacology Wiek van Gilst Pathologie Harry van Goor Department of Medical Biology Subsection Intergrative Genomics Elvira Oosterom Jelle Conradie Ron Korstanje Gerrit van der Steege