Download
1 / 48
520 likes | 1.33k Vues
Chapter 6 PHYSICAL DEVELOPMENT: THE BRAIN, BODY, MOTOR SKILLS AND SEXUAL DEVELOPMENT . AN OVERVIEW OF MATURATION AND DEVELOPMENT. Changes in Height and Weight Rapid increase in height and weight over 1 st 2 years Growth is more gradual during middle childhood

E N D
Chapter 6 PHYSICAL DEVELOPMENT: THE BRAIN, BODY, MOTOR SKILLS AND SEXUAL DEVELOPMENT
AN OVERVIEW OF MATURATION AND DEVELOPMENT • Changes in Height and Weight • Rapid increase in height and weight over 1st 2 years • Growth is more gradual during middle childhood • Puberty (early adolescence) there is another rapid growth spurt
Figure 6.1 Gain in height per year by males and females from birth through adolescence. At age 10 ½ , girls begin their growth spurt. Boys follow some 2 ½ years later and grow faster than girls once their growth begins. BASED ON TANNER, WHITEHOUSE, & TAKAISHI, 1966.
AN OVERVIEW OF MATURATION AND DEVELOPMENT • Changes in Body Proportions • Cephalocaudal – head downward growth • At birth, head and legs each represent 25% of body length • At adulthood, head is 12%, legs 50% • Proximodistal – center outward growth • Internal organs followed by limbs • Trend reverses in puberty – hands and feet followed by limbs, then trunk
Figure 6.2 Proportions of the human body from the fetal period through adulthood. The head represents 50 percent of body length at 2 months after conception but only 12 to 13 percent of adult stature. In contrast, the legs constitute about 12 to 13 percent of the total length of a 2-month-old fetus, but 50% of the height of a 25-year-old adult.
AN OVERVIEW OF MATURATION AND DEVELOPMENT • Skeletal Development • Bones lengthen, thicken, and harden with age completing most growth by 18 • Skull has fontanelles (soft spots for childbirth), and sutures (seams) for expansion for brain growth • Ankles, feet, wrists, hands develop more bones
Figure 6.3 X-rays showing the amount of skeletal development seen in (a) the hand of an average male infant at 12 months or an average female infant at 10 months and (b) the hand of an average 13-year-old male or an average 10-year-old female.
AN OVERVIEW OF MATURATION AND DEVELOPMENT • Muscular Development • Born with all muscle fibers • Increase in density and size, particularly during growth spurt of adolescence • Variations in Physical Development • Structures develop at different rates • Individuals develop at different rates • Cultural variations also exist
Figure 6.4 Growth curves for different body systems. Each curve plots the size of a group of organs or body parts as a percentage of their size at age 20 (which is the 100 percent level on the vertical scale). The “general” curve describes changes in the body’s size as well as the growth of respiratory and digestive organs and musculature. The brain and head grow more rapidly than the body in general, and the reproductive organs are the slowest to reach adult size. (The lymph nodes and other parts of the lymphatic system, which function as part of the immune system, also grow rapidly and actually exceed adult size during late childhood and adolescence.) FROM TANNER, 1962.
DEVELOPMENT OF THE BRAIN • Neural Development and Plasticity • Last 3 prenatal months and first 2 years of life = brain growth spurt • Neurons – basic unit of brain/nervous system; most present at birth • Form synapses (connective spaces) with other neurons • Glia – nourish neurons and encase them in myelin; form throughout life
DEVELOPMENT OF THE BRAIN • Neural Development: Cell Differentiation and Synaptogenesis • Neurons can serve any neural function • Synaptogenesis – formation of synapses • More formed than needed • Roughly half die; some stand in reserve – injury or new skills • Placticity – cells are responsive to experience (allows change in brain)
DEVELOPMENT OF THE BRAIN • Neural Plasticity: The Role of Experience • Reisen – dark reared chimp study • Beyond 7 months, atrophy of retina and optic nerve was irreversible • Increased head circumference in children from high SES homes
DEVELOPMENT OF THE BRAIN • Brain Differentiation and Growth • At birth, brain associated with biological functioning is most developed • Cerebrum and cerebral cortex (higher brain centers) • Primary motor areas; primary sensory areas mature first
DEVELOPMENT OF THE BRAIN • Myelinization • At birth – pathways between sense organs and brain are myelinated • Pathways between muscles and brain are next • Reticular formation and frontal cortex • Needed for long term concentration • Not fully myelinated at puberty
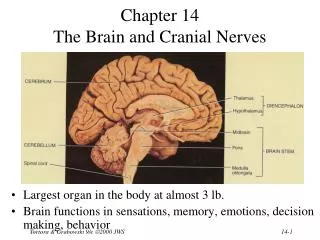
DEVELOPMENT OF THE BRAIN • Cerebral Lateralization • Cerebrum consists of 2 hemispheres connected by the corpus callosum • Each covered by a cerebral cortex • Left – right side of body; speech, hearing, positive emotions • Right – left side of body; music, touch, negative emotions • Lateralization increases with age
Figure 6.6 Lateral view of the left cerebral cortex and some of the functions that it controls. Although the cerebellum and spinal cord are not part of the cerebral cortex, they serve important functions of their own.
MOTOR DEVELOPMENT • Sequence of motor skills is the same for all infants • Large individual variation within children • Rate of motor development not strongly related to future development outcomes
Table 6.1 Age Norms (in Months) for Important Motor Developments (Based on European American, Latino, and African American Children in the United States)
MOTOR DEVELOPMENT • Basic Trends in Locomotor Development • Cephalocaudal – head-downward • Exception is coordination of hip movement before shoulder movement • Due to structure of joints • Proximodistal – center-outward
MOTOR DEVELOPMENT • The Maturational Viewpoint • Motor development is a genetically programmed sequence of events • The Experiential/Practice Hypothesis • Maturation and practice are important • Dynamical Systems Theory • New skills are constructed as infants actively reorganize existing capabilities • Desire is to achieve an objective
MOTOR DEVELOPMENT • Fine Motor Development • Development of Voluntary Reaching • Prereaching is replaced by voluntary reaching • Development of Manipulatory Skills • Claw-like ulnar grasp is replaced by the pincer grasp (near end of first year)
MOTOR DEVELOPMENT • Psychological Implications of Early Motor Development • Motor skills allow for fun social interaction • Provide evidence of normal development • Enhances perceptual, cognitive, and social development • Distance, spatial memory, fear of heights
MOTOR DEVELOPMENT • Beyond Infancy: Motor Development in Childhood and Adolescence • Each year, skills improve • Large muscles, eye-hand coordination • Young children tend to overestimate physical feats they can perform • Puberty – males increase in muscle development; females tend to become less active
PUBERTY: THE PHYSICAL TRANSITION FROM CHILD TO ADULT • The Adolescent Growth Spurt • Begins at about 10 ½ for females • Begins at about 13 for males • Increase in height and weight • Bodies and faces appear more adultlike
PUBERTY: THE PHYSICAL TRANSITION FROM CHILD TO ADULT • Sexual Maturation – • Timed w/growth spurt, predictable pattern • Girls • Onset of breast and pubic hair development • Widening of hips, enlarging of uterus and vagina • Menarche (first menstruation) • Completion of breast/pubic hair growth
PUBERTY: THE PHYSICAL TRANSITION FROM CHILD TO ADULT • Sexual Maturation • Boys • Development of testes and scrotum • Emergence of pubic hair • Growth of penis, ability to ejaculate • Appearance of facial hair • Lowering of voice • Large individual differences in timing
Figure 6.8 Milestones in the sexual maturation of girls (a) and boys (b). The numbers represent the variation among individuals in the ages at which each aspect of sexual maturation begins or ends. For example, we see that the growth of the penis may begin as early as age 10 ½ or as late as 14 ½. FROM TANNER, 1990.
PUBERTY: THE PHYSICAL TRANSITION FROM CHILD TO ADULT • Secular Trends: Are We Maturing Earlier? • Reaching sexual maturity earlier in industrialized societies than in the past • Also growing taller and heavier • Due to • Improved nutrition • Improved health care
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Girls • Hope to be attractive • Worry about height • Reactions to menarche are mixed • Boys • Better body images than girls • More positive about first ejaculation than females are about menarche
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Adolescent Body Image and Unhealthy Weight Control Strategies • Positive body image: • High self-esteem • Positive peer relationships • Body image dissatisfaction: • Teenage depression • Eating disorders • Exercise dependence
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Body image dissatisfaction • Boys • Either want to lose weight, or become more muscular • If average weight, tend to be happy • Girls – compelled to be thin
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Eating Disorders • Anorexia nervosa – • Obsessed with weight gain • Refuse to maintain normal weight • Bulimia nervosa • Binge eating followed by behavior to avoid weight gain • Both more common among females • Peak occurrence between 14 and 18
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Family factors influencing weight behaviors • Chaotic home environment • High conflict levels; low emotionality • Intrapersonal factors • Internalize stress, • Emotionally unexpressive • Behavioral factors • Participation in certain sports • Dieting; perfectionism
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Treatment of Eating Disorders • Family involvement • Realistic views of consequences of actions • Eating family meals • Create environments emphasizing health and fitness, not appearance
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Social Impacts of Puberty • Nonindustrialized societies • Puberty is a sign of adulthood • Marked with formal rites of passage • Other societies • May be an increase in parent-child conflict, but culture and environment influence the experience of adolescence
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Does Timing of Puberty Matter? • Possible Impacts on Boys • Early maturing is beneficial • More confident, social, responsible • Possible Impacts on Girls • Early maturing is a disadvantage • Less outgoing, less popular, attract older males • Many differences fade over time
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Adolescent Sexuality • Hormonal changes increase sex drive • Culture influences sexuality • Education on sexual matters • Preparation for role as a sexual being • Liberal versus restrictive cultures • Western societies – relatively restrictive
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Sexual Attitudes and Behavior • Sexual Attitudes • Becoming more liberal • Sex with affection is acceptable • Decline of the double standard • Sexual Behavior • Sexual activity has increased, more for girls (50% of high school girls, 55% of boys have had intercourse)
Figure 6.9 Historical changes in the percentages of high school students reporting premarital sexual intercourse. DATA FOR FIRST THREE TIME PERIODS ADAPTED FROM DRYER, 1982; DATA FOR MORE RECENT PERIODS FROM BAIER, ROSENZWEIG, & WHIPPLE, 1991; CENTERS FOR DISEASE CONTROL, 1992; REINISCH ET AL., 1992; McKENNA, 1997.
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Personal and Social Consequences of Sex • Factors associated with early sexual involvement • Early maturers from low-income families • Difficulty at school • Sexually active friends • Involved with drug or alcohol abuse • Adolescents fail to use contraception
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Personal and Social Consequences of Sex • Failure to use condoms • Uninformed about reproductive issues • Cannot understand possibility of long-term consequences • Fear of being viewed negatively
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Sexually Transmitted Disease • 20% of adolescents contract one • AIDS fastest growing among those 13 to 19 years old • Teenage Pregnancy and Childbearing • 1,000,000 become pregnant each year • 500,000 babies born to teen mothers • Much higher rate than other countries
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Teenage Pregnancy and Childbearing • Consequences for adolescent mothers • 50% drop out of school • Loss of contact with social network • More likely to be involved in violence • Consequences of babies of adolescents • Intellectual deficits; emotional disturbances; poor peer relations • More delinquent behaviors
THE PSYCHOLOGICAL IMPACTS OF PUBERTY • Dealing with the Problem of Teen Sexuality • Begin at home with communication • Delays onset of sexual relations • Promotes regular condom use • Teen Outreach program • Formal sex ed • Abstinence • Information about contraceptives • Information about resisting pressure
CAUSES AND CORRELATES OF PHYSICAL DEVELOPMENT • Biological Mechanisms • Effects of Individual Genotypes • Set limits for stature, shape, and tempo of growth • Hormonal Influences - Endocrinology of Growth
Figure 6.11 The effect of malnutrition on growth. These graphs show the average heights of Oslo schoolchildren ages 8 to 18 between 1920 and 1960. Notice the trend toward increasing height (in all age groups) between 1920 and 1940, the period between the two world wars. This secular trend was dramatically reversed during World War II (the shaded section of the graphs), when nutrition was often inadequate. FROM TANNER, 1990.
Figure 6.12 Average percentage of excess body weight for obese children who participated in a weight-loss program with and without a parent. ADAPTED FROM EPSTEIN ET AL., 1987.