Digestive System: Liver and Biliary Tract
690 likes | 1.96k Vues
Chapter 16. Digestive System: Liver and Biliary Tract. Digestive System. Consists of 2 tracts: 1. alimentary tract (mouth, pharnyx, esophagus, stomach, large and small intestines)

Digestive System: Liver and Biliary Tract
E N D
Presentation Transcript
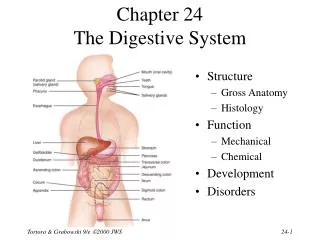
Chapter 16 Digestive System:LiverandBiliary Tract
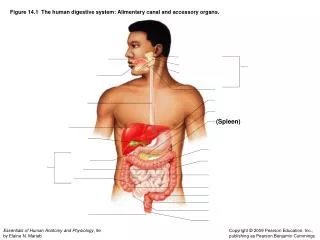
Digestive System • Consists of 2 tracts: • 1. alimentary tract (mouth, pharnyx, esophagus, stomach, large and small intestines) 2. accessory organs contributing to digestion (salivary glands, liver, pancreas, gallbladder, biliary tract) • Both contained in the abdominopelvic cavity which consists of 2 parts • 1. Abdominal cavity-large superior portion • 2. Pelvic cavity-smaller inferior
Abdominal Cavity Extends from diaphragm to superior aspect of pelvis • Stomach • Small & large intestines • Liver/Gallbladder • Spleen • Pancreas • Kidneys
Pelvic CavityLies within margins of pelvis • Rectum/Sigmoid • Urinary bladder • Reproductive organs
Peritoneum • The double-walled serousmembranous sac that encloses abdominopelvic cavity • 1.Parietal Peritoneum- outer portion in close contact with abdominal wall, undersurface diaphragm • 2. Visceral Peritoneum- inner portion-over or around organs • Space between 2 layers is peritoneal cavity
Parietal peritoneum (Adheres to abdominal wall) • Visceral peritoneum- (adheres to organs) • Peritoneal folds • Mesentary and Omentum • Folds caused by adherence of visceral layer of peritoneum • Supports organs in position
Retroperitoneum • Cavity behind peritoneum • Contains kidneys and pancreas
Liver • Largest gland in body • Takes up most of anterior RUQ • Produces 1-3 pints of bile per day
Liver (cont’d) • Falciform ligament divides liver into 2 major lobes • Right lobe • Left lobe • 2 minor lobes • Caudate lobe- part of right lobe -posterior • Quadrate lobe - “ inferior
Liver Physiologic Functions • Formation of bile • Bile: • Aids in digestion of fats • Helps to eliminate waste products of RBC’s collected from liver cells from bile ducts • Also stored in gallbladder
Liver has a dual blood supply • Portal vein (through portal system) • -carries blood from digestive system to be filtered by liver • 2. Hepatic artery • -supplies oxygenated blood from abdominal aorta
Portal System • Consists of veins arising from stomach, intestinal tract, gallbladder and spleen • Blood circulates through these organs rich in nutrients to liver where it is modified before returning to heart via hepatic veins
Biliary System • Consists of : 1. bile ducts 2. gallbladder 3. associated structures involved in production and transportation of bile
2 Primary functions of biliary system: • Drain waste products from liver into duodenum • Help in digestion with controlled release of bile • Bile is greenish-yellow fluid (consisting of waste products, cholesterol, and bile salts) • - excreted from body as feces- gives feces its dark brown color.
Gall bladder • Serves as reservoir for bile from liver – 2oz. capacity (50 percent of bile 1st stored in gallbladder) • Concentrates bile • Helps to break down fats • when food eaten, gallbladder is activated by hormone cholecystokinin which stimulates contraction of gallbladder and releases stored bile into duodenum
Transportation of bile sequence • Liver cells secrete bile- collected by system of ducts flowing from liver through right and left hepatic ducts. • Hepatic ducts drain into common hepatic duct.
Transportation of bile sequence (cont’d) • Common hepatic duct joins with cystic duct from gallbladder to form: • Common bile duct -runs from liver then • Joins with or runs side by side withpancreatic duct into chamber known as • Hepatopancreatic ampulla (or ampulla or vater) • Empties into duodenum • Controlled by Spincter of Oddi (or spincter of hepatopancreatic ampulla)
Biliary Ducts Two main hepatic ducts join to form : • Common Hepatic duct • Unites with: • Cystic duct to form: Common bile duct • Which joins withpancreatic duct and empties into duodenum
Pancreas • Glandular organ • Head will be found within duodenal loop • Generally cannot be seen on radiographs
PancreasCont’d • Both an exocrine and endocrine gland • Endocrine- (Isle of Langerhans) produces glucagon and insulin to regulate sugar metabolism • Exocrine- secretes digestive enzymes that are conveyed through pancreatic duct- often times uniting with common bile duct to hepatopancreatic ampulla then to duodenum
Spleen • Not a part of digestive system • Belongs to lymphatic system • Produces lymphocytes • Stores and removes dead or dying RBC’s • Can be visualized on plain radiographs
Radiography of the Abdomen KUB Flat and upright 3-way abdomen (acute abdomen series - rule out free air, bowel obstruction, infections) • 1. AP • 2. AP upright or left-lateral decubitus (can’t stand) • 3.PA erect chest -to visualize free air under diaphragm
Positioning AP Abdomen • Pt. supine • CR at crest of ilium • Pt. centered at midline • kVp range - 70’s • Expose at end of full expiration
Shielding • 1. If gonads within 2 inches to primary x-ray field even with proper beam limitation • 2. Clinical objectives not compromised • 3. Pt has reasonable reproductive potential
Evaluation Criteria - Abdomen Radiograph • Symphysis pubis to upper abdomen • Vertebral column is centered • Pelvis, ribs, and hips equidistant • No rotation
Evaluation Criteria For Abdomen Radiograph cont’d • Markers must be visible • All soft tissue structures should be present • No motion • Variances in position must beindicated!
Structures Shown On Abdominal Radiography • Size and shape of liver • Spleen • Kidneys • Psoas muscles • Any intra-abdominal tumors, masses, or calcifications
Positioning Variants Of Abdomen Radiograph • Upright • Demonstrates free air under diaphragm • Air-fluid levels • Left Lateral Decubitus • Demonstrates air/fluid levels on non-ambulatory patient
Positioning Variants Of Abdomen Radiograph cont’d • Lateral Position • Demonstrates: • calcification in pre-vertebral space • aneurysms of aorta (if calcified)
Radiography of Biliary Tract & Gallbladder
Radiography Of Biliary Tract & Gallbladder(regular cholecystography) • Cholecystography (largely replaced by Ultrsound, CT, MRI, nuclear medicine) • Study of gallbladder • Oral contrast is used • Cholangiography • Study of biliary ducts • IV contrast is used • May be injected directly into ducts
Biliary Tract Examinations • Why perform? • Determine liver function • Patency and condition of ducts • Demonstrate concentrating and emptying ability of GB • Search for gallstones • Only those that contain calcium are visible
Cholelithiasis (gallstones) Cholecystitis (inflammation of gallbladder) Biliary neoplasia (tumor) Opacities or masses Biliary stenosis (abnormal narrowing) IndicationsforBiliary Tract Exam
ContraindicationsforBiliary Tract Exams • Allergy to contrast • Pyloric obstruction (blockage from stomach to duodenum) • Severe jaundice • Malabsorption • Liver dysfunction • Hepatocellular disease
Patient Prep • Fat-free meal evening before • Oral contrast taken 2 to 3 hours before evening meal • NPO after midnight until exam • Early morning appointment • Ensure that patient can, will, and did follow instructions
Gallbladder Exam(Cholecystography) • Obtain scout film • Full KUB or RUQ film • Determine contrast is in gallbladder and is visible • May include fluoroscopic examination • Post-fatty meal film may be obtained • Determines emptying ability of GB
Position of Gallbladder • RUQ • In hypersthenic pt. • Superior and lateral • In Asthenic • Inferior and nearer to spine
PA Projection • Patient prone recumbent or prone upright • Center 10x12 cassette at RUQ, level of the elbow • 70 - 80 kVp range • Exposure made at end of full expiration
PA Oblique Projection • LAO position • Pt rotated 15 - 40 degrees depending on body habitus • CR at level of elbow, between spine and midaxillary line 10x12 cassette
Rt. Lateral Decubitus • Position • Rt. Lateral recumbent • Central Ray • Directed horizontally to level of gallbladder • Good for non-ambulatory patients
Gall Bladder cont’d • Must be free of foreshortening or superimposition from itself and adjacent structures • Entire gallbladder must be visualized • No motion or rotation
Very rarely performed Used when patients cannot tolerate oral contrast Generally done in supine, and RPO positions Films taken at timed intervals - up to about 40 minutes after injection Tomography may be used Intravenous Cholangiography (IVC)
Percutaneous Transhepatic Cholangiography(performed preoperatively) • Percutaneous: any medical procedure where access to inner organs or other tissue is done via needle-puncture of the skin, rather than by scapel • Pt prepped for sterile procedure • Chiba (long) needle is placed into bile ducts • Contrast is injected under fluoro • AP Projections obtained • Biliary drainage or stone extraction may accompany this procedure
CholangiographyIntra-operative • Obtained during a cholecystectomy • Pt. prepped and draped for surgery • Examines patency of ducts during or after surgical removal of GB
Procedure for Operative Cholangiography • Obtain scout of RUQ when possible • A grid should be used • C-Arm may be used for a dynamic study • May need to rotate patient into RPO • Coordinate exposures w/anesthesiologist
T-Tube Cholangiography • Post-operative procedure- performed through T-tube left in common hepatic and common bile ducts • Determines patency (open) of biliary ducts after cholecystectomy, status of Spincter of oddi, residual or undetected stones
T-Tube Cholangiography (cont’d) Procedure: • Obtain scout of RUQ • Contrast will be injected into T-tube • Obtain AP and RPO films
Cholangiogram types Percutaneous Intraoperative T-Tube