Understanding Hemolytic Anemia: Causes, Types, and Treatment Options
330 likes | 551 Vues
Hemolytic anemia is characterized by the excessive destruction of red blood cells (RBCs), leading to various symptoms such as jaundice, fatigue, and dark urine. It can be classified into acute and chronic forms, with congenital and acquired causes. Immune-mediated and non-immune factors drive the condition, including autoimmune disorders and certain toxins. Diagnostic signs include low haptoglobin, elevated bilirubin, and reticulocytosis. Treatment varies based on the underlying cause and may include corticosteroids, transfusions, and immunosuppressive therapies.

Understanding Hemolytic Anemia: Causes, Types, and Treatment Options
E N D
Presentation Transcript
Hemolytic anemia Excessive destruction of red cells Acute Hemolytic anemia Chronic Hemolytic anemia Congenital Acquired : Immune Non-immune
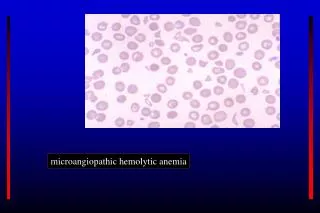
Classification of hemolytic anemia - Intravascular hemolytic anemia : - Turbolent and Marsch hemoglubinuria • Fibrin deposetion : DIC , TTP , UHS (Microangiopathic ) • Complement lysis : PNH , PCH , • and Non - compatible blood transfusion - Enzymppathies: G6PD D. , Pyrovate Kynase.d. - Toxin : colestidium velshay bacter - Extravascular hemolytic anemia RBC desruction by : - Immune Liver - Membran defect Spleen Other tissues
Laboratory Signs of Accelerated Red Cell Destruction - Decreased erythrocyt life span - Increased catabolism of heme. 1- Hemoglbinemia 2- Hemoglobinuria 3- Hemosiderinuria 4- Methemalbumineuria 5- Absent Haptoglobin 6- Reduced serum hemopexin level • Fall in blood hemoglobin level at a rate greater than • 1.0 g/dl/week
In the chronic hemolytic anemia • - quite severe anemia • can be tolerated with symptoms only arising on exercise. • -The patients jaundiced but this is oftenmild. • The urine is dark especially after standing • The spleen tend to be enlarged to degree of the underlying cause of the hemolysis . • - Leg ulcer usualy over the lateral malleolus
Immune-Mediated Hemolytic Disorders 1- IgG warm autoantibodies: IgG bind to RBC at 37c but fail to agglutinate the RBC. 2-Cold agglutinins: almost always are are of the IgM subtype and clump RBC at cold temperatures. 3- Donath-Landsteiner ( IgG) antibodies. Antibodies bind to RBC membranes in the cold and activate the Hemolyitic complement cascade .
Laboratory features of hemolytic anemia - Raised level of unconjugated bilirubin - Reticulocytosis - Urine hemosiderinuria - Red cell survival studies with C-labelled - Erythroide hyperplasia in bone marrow - Examination of peripheral blood smear - Direct antiglobulin test ( Coombs test ) - Absent haptoglubin - Hemoglubinemia and hemoglubinuria
The Antiglobulin ( Coombs” ) Test The test for routine detection of immunohemoiytic anemia , used most widely is the direct antiglobulin or Coombs” test. Positive results indicated thet the red cells are coated with IgG and / or complement components, especially C3. 2- 5 % of patients with immuno-hemolytic disease have negative test results because the amount of globulin on the cell surface is below the detection limits.
The Osmotic Fragility Test The Osmotic F.T. is a measure of the resistance of erythrocytes to hemolysis by osmotic stress . The test consists of exposing red celle to decreasing strengths of hypotonic saline Solutions and measuring the degree of hemolysis. Normally , hemolysis begin 0.45 to 0.50 g/dl and at which it is complete normally 0.30 to 0.33 g / dl. Increased fragility is indicated by a shift of the curve to the left or high value for median corpuscular fragility ( MCF ).
Chronic Congenital Hemolytic Anemia - Various degree of anemia - Jaundice - Crises - Splenomegaly - Cholelithiasis - Leg Ulcers - Skeletal Abnormalities
Hemoglubin defects • Defects of synthesis : • the thalassemias syndrome. - Defects of structure : Sickle cell disease.
Acute Hemolytic anemia Congenital Acquired : Immune Non-immune
Etiology of Hemolytic anemia 1- Congienital : Defect of Hemoglobin synthesisand structure Thalassemia Sickle cell disease Unstable hemoglobins Membrane defects Hereditary spherocytosis Hereditary elliptocytosis Red cell enzyme defects G6PD deficiency Pyruvate kinase deficiency 2- Acquired (Non-Immune) 3- Acquired ( immune )
Etiology of Warm –antibody type autoimmune Hemolytic A. Idiopatic (primary) Secondary : 1- Lymphoprolifrative diseasee, CLL ,NHL…. 2- Connective tissue diseases ,SLE,variable immunodeficiency 3- Immune deficiency disorders,AIDS, common variable imm.d. 4- Druges induced immuno-hemolytic anemia: penicilline , Quinidine , Methyldopa , Cephalosporine
Treatment of warm autoantibodu H.A. If mild ,no specific therapy may needed. Treatment of secondary causes ,underling diseases. When treat underling diseases Unsuccessful: - Folic acid and Vit B12 - RBC transfusions - Corticosteroids - Splenoctomy - IV immunoglobulin • Immunosupressive therapy - Danazol and Vinca alkaloids
Treatment of warm autoantibodu H.A. If mild ,no specific therapy may needed. Treatment of secondary causes ,underling diseases. When treat underling diseases Unsuccessful: - Folic acid and Vit B12 - RBC transfusions - Corticosteroids - Splenoctomy - IV immunoglobulin • Immunosupressive therapy - Danazol and Vinca alkaloids
- Folic acid and Vit B12 - RBC transfusions - Corticosteroids - Splenoctomy - IV immunoglobulin • Immunosupressive therapy - Danazol and Vinca alkaloids