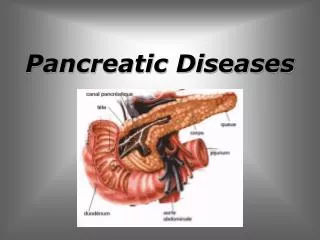
Pancreatic diseases
Pancreatic diseases. WU JIAN Department of hepatobiliary Surgery First Affiliated Hospital Zhejiang University School of Medicine. Pancreas: Anatomy and Physiology. Retroperitoneal organ 15-20cm in length Head, neck, body and tail

Pancreatic diseases
E N D
Presentation Transcript
Pancreatic diseases WU JIAN Department of hepatobiliary Surgery First Affiliated Hospital Zhejiang University School of Medicine
Pancreas: Anatomy and Physiology • Retroperitoneal organ • 15-20cm in length • Head, neck, body and tail • Uncinate process: curves behind the superior mesenteric vessels
Neighborhood of the pancreas • Posterior L1-2 vertebral column • Anterior stomach, omentum • Right Duodenum • Left Splenic hilum
Main duct : Wirsung ( 1642) Ampula: Vater (1720) Accessory duct : Santorini( 1734)
Pancreas: blood supply • HEAD: Superior pancreatoduodenal A. (from gastroduodenal A.) Inferior pancreatoduodenal A. (from SMA) • BODY AND TAIL: superior pancreatic A. pancreatic magna A. transverse pancreatic A. • VEIN: to splenic vein ,SMV and portal vein
Common pathway
Physiology • Exocrine:pancreatic juice。 • HCO3- and digestive enzyme • Endocrine: • A cell:glycagon • B cell:insulin • D cell :somatostatin • G cell :gastrin
Acute Pancreatitis Chronic Pancreatitis Pancreatic cancer Periampullary cancer Endocrinal tumor
AcutePancreatitis • Common acute abdomen • Local inflammatory change in pancreas • Systemic change • Life-threatening inflammatory disorder of the pancreas • Abrupt onset and unpredictable course • Variable severity and duration • Self-limited but remarkable morbidity and mortality
Etiology • Biliary tract disease • Abuse of ethanol • Endoscopic retrograde cholangiopancreatography • Trauma and operation • Ischemia of pancreas • Drugs • Idiopathic pancreatitis • Hypercalcemia • Hyperlipidemia • Infections and Parasites • Scorpion sting
PATHOGENESIS • “Self digestion” • Reflux of bile or duodenal juice • Trypsinogen was activated • Trypsin can activate the other zymogens • Intraparenchymal enzyme activation, tissue destruction, and ischaemic necrosis.
Pathological and clinical type • Pathological type • Acute edematic pancreatitis • Acute hemorrhgic and necrotic pancreatitis (AHNP) • Clinical type • Mild Acute pancreatitis (MAP) • Severe Acute pancreatitis (SAP) • Fulminant Acute pancreatitis (FAP)
Clinical manifestations • Abdominal pain • Nausea, vomiting • Distension • Tenderness, rebound tenderness, muscular regard • Fever,jaundice, • Gray-Turner sign: flank ecchymoses Cullen sign: periumbilical ecchymoses • MODS
laboratory test • Amylase level in serum and in urine • Lipase assays • Blood Rt, liver function, FBS, PaCO2 ,serum calcium, DIC • Diagnostic paracentesis
Image findings • BUS • CT • ERCP • MRCP • Abdomen plain film
Local complication • Pancreatic necrosis • Infective pancreatic necrosis • Sterile pancreatic necrosis • Pancreatic abscess • Pancreatic pseudocyst
Acute pancreatic pseudocyst • Peripancreatic fluid collections occur in 10-20 % of patients • Those persisting beyond the phase of acute inflammation become pancreatic pseudocysts • Collection surrounded by fibrous tissue or granula tissue • Diagnosed by PE or image test • Round or ellipse • Clear cyst wall
Severe Acute Pancreatitis • Severe Acute pancreatitis (SAP) • Complicated with MODS • Necrosis, abscess, pseudocyst • Or both
Classificationsystem • General evaluation • John Ranson score (1974):5 (on admission) +6 (48hr) • Imrie score:8 (WBC,Ca,sugar,PO2,LF) • APACHE II score (1985):12+age+Chronic health+coma • Atlanta classification system(1992) • Local evaluation • Beger’ criteria (1985) • Balthazar CT classification system (1990):I, II, III GRADE • MODS evaluation • Marshall MODS score system(1995):6 systems/organs involved
Clinical manifestation of SAP • Abdominal sign: obvious tenderness, rebound tenderness, muscular regard, distension, lose of bowl sound • Mass in abdomen, Grey-Turner, Cullen • MODS • Irreversible shock • CT: swelling,uneven density, invade to outside of pancreas(Balthazar CT>II) • APACHE value>8
MODS • Cardiac function:quick pulse、shock • Pulmonary function :PaO2<60mmHg,ARDS • Liver function:jaundice, elevated ALT • Renal function:elevated BUN and Creatinine • Digestive function:GI bleeding • Endocrinal function :glucose>11.1mmol/L • Coagulation system:DIC • Nerve system:unclear consciousness、pancreatic brain disease
Stage of SAP • Acute response stage:within 2 weeks • complicated with shock,ARDS,renal failure • Systemic infection stage:2weeks to 2 months • Bacteria or fungus infection • Post-infection stage:after 2 3 months • Abscess, fistula,
Acute Response Stage • ICU :to prevent MODS • fasting the patient, nasogastric suction • Minimizing pancreatic secretion • antacids • 5-FU • somatostatin analogues • antiprotease • Fluid replacement and Nutritional support • maintenance of adequate hydration • TPN,glucose ,lipid, amino acid, protein • Analgesia • Antibiotics • Traditional Chinese Medicine • Abdominal lavage
Indication of Operation • Biliary obstruction • Secondary pancreatic infection • Shock cannot be reversed, multiple ogan deteriorate • Undetermined diagnosis, need to laparotomy
Principle for treatment of pancreatitis SAP MAP Biliary Non-biliary Conservative therapy No infection Obstuctive Non-obstructive Infection Urgent operation Or ERCP Elective operation Conservative therapy Elective operation Conservative therapy
Chronic pancreatitis • Recurrent upper abdominal pain • With dysfunction of endocrine and exocrine of pancreas
Clinical manifestition • Four main symptoms • Abdominal pain • Body weight loss • Diabetes • Lipid diarrhea
Therapy of chronic pancreatitis Relieve pain Drainage of the pancreatic juice Prevent acute attack Ameliorate the nutrition Improve pancreatic function Non-operation or operation
Pancreatic Cyst • Pancreatic pseudocyst • Congenital pancreatic cyst • Retention pancreatic cyst • Neoplastic pancreatic cyst • Pancreatic cystadenoma • Pancreatic cystadenocarcinoma
Pancreatic pseudocyst • Indication for operation • Associated with ongoing pain • More than 6 cm in diameter which persist for 6 weeks • Cyst with haemorrhage and sepsis • Methods • Percutaneous drainage • Operative drainage • Cystgastrostomy, cystjejunostomy • Resection of pancreatic body and tail