Download
1 / 68
1k likes | 2.92k Vues
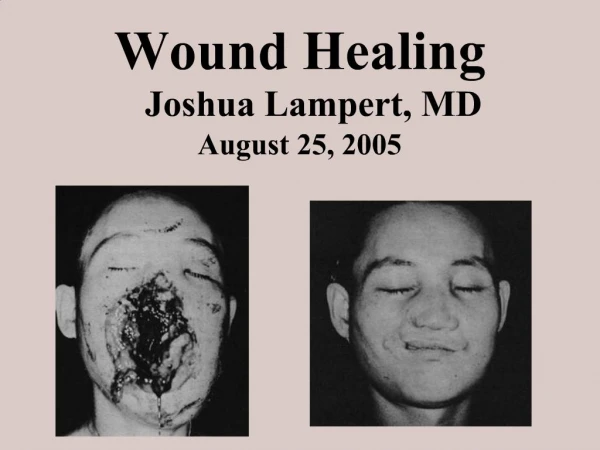
Acute and chronic inflammation. Repair: cell growth and regeneration. Wound healing. . 2011. Acute inflammation. is early, immediate, response of vascularized living tissue to local injury, non-specific its purpose is 1) to destroy injurious agent

E N D
Acute and chronic inflammation. Repair: cell growth and regeneration. Wound healing. 2011
Acute inflammation • is early, immediate, response of vascularized living tissue to local injury, non-specific • its purpose is • 1) to destroy injurious agent • 2) to reconstitute a damaged tissue (healing) • repair already begins during early phases of inflammation • injured tissue is replaced by regeneration of parenchymal cells • by connective tissue formation -scarring
Causes of inflammation • microbial infections: bacteria, viruses, fungi, etc. • hypersensitivity reactions • physical agents: burns, UV light, radiation, trauma • chemical agents: acids, alkalis, oxidising agents, toxins, endotoxins, even toxic catabolites derived from endogenous processes, such as in uraemia, etc. • tissue necrosis: ischemia
Main clinical signs and symptoms of inflammation • Acute inflammation is characterised by five major signs described by Celsus and Virchow • rubor = redness from dilatation of blood vessels • calor = increased heat and fever- redness and heat -due to an increased rate and volume of blood flow because of vasodilatation, release of pyrogens • tumor= swelling from edema • dolor= pain form oedema and histamine release, pain is said to be due to an accumulation of acid metabolites that stimulate nerve endings • functio laesa = loss of function form pain and swelling
Morphologic and functional changes in acute inflammation • microcirculatory response • cellular response
CELLS OF THE INFLAMMATORY RESPONSE • Neutrophilic leukocytes • leukocytes are the first cells to appear at the site of acute inflammation • is to degrade cell debris and to ingest and kill microbes- phagocytosis • Eosinophilic leukocytes • associated with hypersensitivity responses • Basophils and mast cells • mast cells are usually seen in tissues in type I hypersensitivity reactions mediated by IgE • binding of IgE to the receptor on mast cells and basophils leads to degranulation of granules and release of the granule contents (heparin, histamine, and enzymes, such as acid hydrolase) into the tissues
Monocytes and macrophages • macrophages are major scavenger cells of the body • enzymes, such as lysozyme and hydrogen peroxide- degrade particulate material including micro-organisms • they control many of the cellular, vascular and reparative responses of inflammation by releasing chemotactic factors, cytokines (tumour necrosis factor) and growth factors (PDGF) and transforming growth factor beta (TGF-beta) • Lymphocytes and plasma cells • these are principal cells of specific immune responses- produce antibodies
Microcirculatory response • increased blood flow and permeability of blood vessels • Vasodilatation leads to hyperaemia (= increased amount of blood in infl. area )- heat and redness • increased permeability of blood vessels- associated with slowing of the circulation- called stasis • increased passage of fluid out of microcirculation because of increased permeability in acute inflammation = exudation of fluid • vascular leakage- loss of protein-rich fluid from blood vessels • reduction of osmotic pressure within blood vessels • increase in interstitium- accumulation of fluid out of blood vessels • inflammatory oedema- major feature of acute inflammation
The major local manifestations of • acute inflammation, compared • to normal. • Vascular dilation • extravasation of plasma fluid and proteins (edema) • leukocyte emigration
Composition of inflammatory exudate • exudate is fluid • rich in plasma proteins (albumins, immunoglobulins, fibrinogen) • converted into fibrin by tissue tromboplastin • Fibrin can be recognised microscopically-pink fibres or clumps, macroscopically- most easily seen on acute infl. of serosal surfaces-acute fibrinous pericarditis- „bread and butter„ appearance. • Transudation= increased passage of fluids (very low level of plasma proteins, and no cells) through blood vessels with normal permeability- increased hydrostatic pressure or decreased plasma osmotic pressure -composition similar to ultrafiltrate of plasma
Significance of the process of exudation • Exudation • helps to destroy infectious agent by its diluting • by flooding the area with blood rich in immunoglobulins and other important defensive proteins • by increasing lymphatic flow -lymphatic drainage may to spread infectious agents • acute inflammation of lymphatics= lymphangitis • acute inflammation of lymph nodes= lymphadenitis
Cellular response • NEUTROPHILIC LEUKOCYTES • remain predominant cell type for several days in acute inflammation. • emigration of neutrophils -leukocytes actively leave the blood vessel by moving through dilated intercellular junctions, pass through basement membrane and reach the extracellular space • MACROPHAGES • LYMPHOCYTES • movements of these cells are similar to that of neutrophils- chemotactic mediators for macrophages- complement factor C5 and lymphokines (secreted by lymphocytes) • ERYTHROCYTES enter extracellular space passively – • RBCs are pushed out from the blood vessel by hydrostatic pressure- the process is called erythrodiapedesis • when large numbers of erythrocytes enter the inflamed area = haemorrhagic inflammation
Major events in phagocytosis • recognition and attachment of bacteria by the phagocytic cells - either directly (large inactive particles) or after opsonization (antigen is coated by opsonins) • engulfment - extensions of cytoplasm (pseudopods) flow around the particles - formation of phagocytic vacuole, this vacuole fuses with membrane of lysosomal vacuoles-degranulation of leukocytes • bacterial killing and degradation-killing of bacterial organisms is accomplished by activities of reactive oxygen species • Failure of oxidative metabolism during phagocytosis - leads to a severe disorder of immunity = in chronic granulomatous disease of childhood
MORPHOLOGIC PATTERNS IN ACUTE INFLAMMATION • Serous inflammation • is characterised by abundant serous exudate • derived either from the blood stream or from the secretory activity of mesothelial cells • pleural or pericardial cavities, skin, mucosal surfaces • serous exudate is easily removed- complete regeneration
Acute inflammation • Serous
Fibrinous inflammation • Caused by more serious injuries • permeability of blood vessel is greater • and more proteins including large molecules of fibrinogen pass the vascular wall • Fibrinous exsudate can be removed-process calledresolution • when fibrinous exsudate is not removed • fibrin may stimulate the ingrowth of fibroblasts into the blood vessel wall, thus leading to scarring- this process is called organization
Acute inflammation • Fibrinous
Suppurative or purulent inflammation • is characterized by production of large amounts of purulent exsudate (pus) • Abscess localized collection of purulent exudate • Ulcer = is a local defect in the tissue, mainly in the mucosal or cutaneous surfaces
Acute inflammation • Purulent (suppurative)
Purulent-suppurative inflammation Bronchopneumonia
Acute inflammation • Purulent (suppurative) peritonitis
Ulcerative, pseudomembranous inflammation • acute ulcer- intense leukocyte infiltrate and vascular dilatation in the margins • chronic ulcer-more developed fibroblastic reaction, scarring and infiltration of lymphocytes, macrophages and plasma cells
Fibrinopurulent and pseudomebranous Pseudomembranous colitis
SYSTEMIC CLINICAL SIGNS OF ACUTE INFLAMMATION • fever • results either of direct activity of cytokines or through local activity of prostaglandins • changes in the peripheral white blood cells • leucocytosis- the total number of neutrophils in the peripheral blood is increased • is common feature especially in bacterial infections • „ shift to the left“ means an increased number of immature neutrophils in peripheral blood • Leukocyte count-may reach levels of about 15 or 20 thousands cells per mm3- extreme levels (more than 40 thousand)- referred to as leukemoid reaction • viral infections tend to produce neutropenia (decreased number of leukocytes) with lymphocytosis (excess of lymphocytes in the blood)
CHRONIC INFLAMMATION • acute inflammation usually disappears after a few days and tissue returns to normal • Complete resolution -means total restoration and regeneration of injured area. • Healing by scarring -occurs after tissue destruction, in case of tissue defects, with abundant fibrin leakage, secondary infection, • Progression to chronic inflammation • chronic inflammatory response may follow acute inflammation that failed to destroy injurious agent or may be chronic from the onset (without a clinically apparent acute phase)
Outcomes of acute inflammation: resolution, healing by scarring, or chronic inflammation
Causes of chronic inflammation • persistent infection - caused by distinctive infectious agents, such as mycobacterium, treponema pallidum, some fungi, by organisms of lower toxicity, by intracellular organisms • prolonged exposure to undegradable material, such as silica particles, carbon particles which, after being inhaled, set up a chronic inflammatory response in lungs • autoimmune diseases= immune reaction set up against own tissues or cells - reveal a chronic inflammatory pattern- for example rheumatoid arthritis
MORPHOLOGIC FEATURES AND CLINICAL SIGNS OF CHRONIC INFLAMMATION • chronic inflammation is an inflammatory response • characterized by the presence of lymphocytes, plasma cells and macrophages • it is distinguished from acute inflammation • by the absence of cardinal signs such as rubor, calor, dolor, tumor • active hyperemia, fluid exudation and neutrophilic emigration are absent • it is distinguished from acute inflammation by its long duration, which permits a manifestation of immune response • Often associated with scarring, fibroproliferation
chronic acute
Histologic hallmarks of chronic inflammation • infiltration by macrophages, lymphocytes and plasma cells • proliferation of fibroblasts and myofibroblasts and proliferation of small blood vessels, together known as formation of granulation tissue • in most cases, the process of chronic inflammation is accompanied by a proliferation of connective tissue (deposition of collagen fibres), referred to as fibrosis • usually marked tissue destruction
Granulation tissue Reparation component of inflammation is represented by granulation tissue composed of budding capillaries, fibroblasts and occasional inflammatory cells
CHRONIC INFLAMMATORY CELLS • MACROPHAGES • play central role in chronic inflammatory infiltrate-macrophages are the most effective phagocytic cells in acute and chronic inflammatory response • enzymatic degradation and phagocytic activity • following activation-macrophages produce biologically active products, such as: • enzymes - neutral and acid proteases • chemotactic factors for leukocytes • growth factors and promoting factors for fibroblasts and blood vessels- thus macrophages may modulate a formation of non-specific granulation tissue • cytokines, such as interleukin I , TNF,etc.
PLASMA CELLS • produce antibodies directed against persistent antigens or against altered tissue components • LYMPHOCYTES • when activated by the contact with antigen, lymphocytes release lymphokines- many of them stimulate macrophages • on the other hand, lymphocytes may be stimulated by cytokines released by activated macrophages • EOSINOPHILS • are characteristic of immunologic reaction mediated by IgE and of parasitic infections
NEUTROPHILIC LEUKOCYTES • in chronic inflammation of bone marrow (osteomyelitis)- large numbers of neutrophils may persists for months • also chronic inflammation of fallopian tube may have the pattern of chronic suppuration with large numbers of neutrophils • FIBROBLASTS • fibroproduction and accumulation of extracellular proteins- characteristic features of chronic inflammatory response
MORPHOLOGIC TYPES OF CHRONIC INFLAMMATORY RESPONSE • GRANULOMATOUS CHRONIC INFLAMMATION • is characterized by formation of epithelioid granulomas • granuloma- is defined as an aggregate of macrophages, two types of granulomas are recognised • epithelioid granuloma- represents immune response • macrophages are activated by T-lymphocytes • „ epithelioid cell“ are activated macrophages - large cells with abundant pale foamy cytoplasm - superficial resemblance to epithelial cells • typical feature of epithelioid granulomas is formation of Langhans-type giant cells- are derived from macrophages
Chronic granulomatous inflammation Langhans cell Epithelioid histiocytes Granuloma (also called „specific granulation tissue“) is composed of modified macrophages)
Epithelioid granulomas occur in • infection due to intracellular organisms • Tuberculosis (Mycobacterium Tuberculosis) • Leprosy (Mycobacterium leprae) • Syphilis (Treponema pallidum) • Cat-scratch disease (Gram negative bacillus)-rounded or stellate granulomas usually within lymph nodes containing the central granular debris and leukocytes • Several parasitic and fungal infections (schistosomiasis, cryptococcus) • Sarcoidosis (Mycobacterium) • disorders due to chemical agents such as beryllium (berylliosis) • Crohn disease
Tuberculosis • Tuberculosis is characterized by specific granulomas, caseous necrosis and finding of Mycobacterium tuberculosis (Ziehl-Nielsen stain)
Chronic granulomatous inflammation • Sarcoidosis ?allergic reaction to the presence of non-virulent mycobacteria?
Chronic granulomatous inflammation • Sarcoidosis Asteroid inclusions Schaumann´s inclusions Granuloma without caseous necrosis Hamazaki – Wesenberg inclusions