Download
1 / 116
1.17k likes | 1.42k Vues
MORPHOLOGICAL REACTIONS TO ACUTE AND PERSISTENT STRESS HEALING REPAIR REGENERATION NEOPLASIA. C ellular reaction var ies depending on the type duration and severity of injury. Adaptation a trophy h ypertrophy h yperplasia m etaplasia d ysplasia. HYPERTROPHY HYPERPLASIA.

E N D
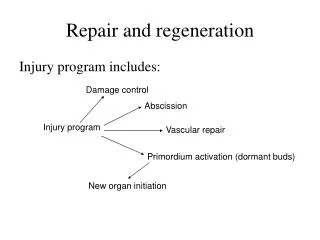
MORPHOLOGICAL REACTIONS • TO • ACUTE AND PERSISTENT • STRESS • HEALING • REPAIRREGENERATION • NEOPLASIA
Cellular reaction varies depending on the type duration and severity of injury
Adaptation atrophy hypertrophy hyperplasia metaplasia dysplasia
HYPERTROPHY HYPERPLASIA
HYPERPLASIA and HYPERTROPHY are two distinct processes but frequently both occur together
HYPERPLASIA takes place by contrast HYPERTROPHY involves _______________________________________
HYPERTROPHY The increased size of the cells is due not to cellular swelling but to the synthesis of more structural components.
HYPERTROPHY -physiologic -pathologic __________________________________ caused by increased functional demand or by specific hormonal stimulation
- increased workload -hormonal stimulation
HYPERPLASIA andHYPERTROPHY often occur concomitantly during the responses of tissues and organs to increased stress and cell loss even cardiac and skeletal muscles are capable of limited proliferation as well as repopulation from precursors
MECHANISMS OF HYPERTROPHY • (cardiac muscle hypertrophy) • many signal transduction pathways • induction of a number of genes • stimulation of synthesis of cellular proteins
GENES INDUCED DURING HYPERTROPHY
- switch of contractile proteins from adult to fetal or neonatal forms - some genes that are expressed only during early development are re-expressed in hypertrophic cells
TRIGGERS FOR HYPERTROPHY • IN THE HEART • -mechanical triggers • -trophic trigger
HYPERTROPHY eventually reaches a limit
The limiting factors for continued hypertrophy and the causes of the cardiac dysfunction are poorly understood
HYPERPLASIA increase in the number of cells in an organ or tissue, usually resulting in increased volume of the organ or tissue
PHYSIOLOGIC HYPERPLASIA hormonal hyperplasia compensatory hyperplasia wound healing s
In hormonal hyperplasia, In compensatory hyperplasia
Although these forms of hyperplasia are abnormal, the process remains controlled, because the hyperplasia regresses if the hormonal stimulation is eliminated That distinguishes benign pathologic hyperplasiasfrom cancer, in which the growth control mechanisms become defective.
PATHOLOGIC HYPERPLASIA constitutes „a fertile soil in which cancerous proliferation may eventually arise.”
METAPLASIA a reversible change in which one adult cell type (epithelial or mesenchymal) is replaced by another adult cell
epithelial metaplasia columnar to squamous
the influences that predispose to metaplasia if persistent, may induce malignant transformation ofmetaplasticepithelium
epithelial metaplasia squamous to columnar type Barrett esophagus
precursor cells differentiate along a new pathway
Certain cytostatic drugs cause a disruption of DNA methylation patterns and can transform mesenchymal cells from one type to another
what does it mean: • tumour • neoplasm • cancer • carcinoma
TUMOR originally - swelling caused by inflammation tumor = neoplasm (leukemia is not a tumor )
ONCOLOGY CANCER
"A neoplasm • is an abnormal mass of tissue*, • the growth of which exceeds • and is uncoordinated • with that of the normal tissues • and • persists in the same excessive manner • after cessation of the stimuli • which evoked the change."
All* neoplasms have two basic components: • (*almostall) • - proliferating neoplastic cells = parenchyma • - supportive stroma • made up of connective tissue • and blood vessels • neoplasms are critically dependent • on their stroma
desmoplasia scirrhous
NOMENCLATUREOF TUMORS is based on the parenchymal component _______________________________ tumors are designated by attaching the suffix -oma to the cell of origin
Benign Malignant fibroma chondroma osteoma lipoma fibrosarcoma chondrosarcoma osteosarcoma liposarcoma Epithelial Non-epithelial adenocarcinoma squamous cells carcinoma adenoma papilloma
BENIGN TUMORS e.g.
MALIGNANT TUMORS sarcomas malignant tumors arising in mesenchymal tissue
carcinomas malignantneoplasms of epithelial cell origin
Not infrequently a neoplasm is composed of undifferentiated cells of unknown tissue origin and must be designated merely as „a poorly differentiated” or „undifferentiated malignant tumor”
polyp macroscopically visible projection above a mucosal surface
look at the following slides, recognise the tissue of origin and name the neoplasms
DIFFERENTIATION the extent to which neoplastic cells resemble comparable normal cells, both morphologically and functionally
well-differentiated tumors poorly differentiated or undifferentiated tumors