Download
1 / 33
660 likes | 2.31k Vues
Oxygen and Carbon Dioxide transport in the blood. Majority of O 2 and CO2 is transported in the blood by: O2 combing with hemoglobin CO2 transformed into bicarbonate (HCO 3 ¯). Hemoglobin and O 2 transport. ±99% of O 2 transported in blood is chemically bound to hemoglobin

E N D
Majority of O2 and CO2 is transported in the blood by: • O2 combing with hemoglobin • CO2 transformed into bicarbonate (HCO3¯)
Hemoglobin and O2 transport • ±99% of O2 transported in blood is chemically bound to hemoglobin • Hemoglobin is a protein found in red blood cells (erythrocytes) • Each hemoglobin molecule can hold up to 4 O2 molecules
O2 combined with hemoglobin = oxyhemoglobin • O2 that is NOT combined with hemoglobin = deoxyhemoglobin
The amount of O2 that can be transported depends on the concentration of hemoglobin • Normal, healthy men = 150g/L of blood • Normal, healthy women = 130g/L of blood • When a hemoglobin molecule is completely saturated with O2 it can transport 1.34ml of O2
Therefore if hemoglobin if full (100% saturated with O2): • Healthy male can transport 200ml of O2 • Healthy female can transport 174ml of O2 • 100% saturation occurs at sea level (low altitude)
Partial Pressure • The amount of O2 bound to hemoglobin is directly related to the partial pressure of O2. • PO2: All gases exert pressure on the walls of their container because the molecules of gas bounce off the walls. • Partial pressure is used to describe a mixture of gases. • Defined as the pressure that any one gas would exert on the walls of the container if it were the only gas present
In the lungs, where the alveoli and capillaries exchange gases, PO2 is high • Therefore O2 binds instantly to hemoglobin. • As the blood circulates to other body tissue the PO2 becomes lower • Therefore hemoglobin releases O2 into the tissue because the hemoglobin cant maintain its full capacity of O2
Oxyhemoglobin Dissociation Curve • In the alveolar capillaries in the lungs: • O2 binding with hemoglobin is called loading • Release of O2 from hemoglobin is called unloading • Loading & unloading are reversible actions: Deoxyhemoglobin + O2 Oxyhemoglobin
Oxyhemoglobin Dissociation Curve • An important tool for understanding how our blood carries and releases oxygen. • Relates oxygen saturation (SO2) and partial pressure of oxygen in the blood (PO2) • Determined by what is called "hemoglobin's affinity for oxygen“ how readily hemoglobin acquires and releases oxygen molecules from its surrounding tissue.
Oxygen Dissociation Curve • Shows the percentage of O2 that is bound to hemoglobin at each O2 pressure. • The curve is S-shaped with a steep slope between 10 and 60 mmHg and a flat portion between 70 and 100 mmHg. • At rest the body’s O2 requirement is low & only ±25% is unloaded into muscles • At intense exercise, PO2 can reach 20mmHg and 90% of O2 is unloaded into muscles
Significance of the Flat Portion • The flat portion of the curve shows that the PO2 can fall from 100 to 60 mmHg and the hemoglobin will still be 90% saturated with O2 • At pressures above 60mm Hg, the dissociation curve is relatively flat. • This means the O2 content does not change much (even with large changes in the partial pressure of oxygen) • E.g. PO2 can fluctuate between 90 – 100mmHg without a large drop in the percentage of hemoglobin that is saturated with O2 • *This is important because there is a drop in PO2 with aging and with climbing high altitudes
Haemoglobin Saturation at High Values Lungs at sea level: PO2 of 100mmHg haemoglobin is 98% SATURATED Lungs at high elevations: PO2 of 80mmHg, haemoglobin 95% saturated When the PO2 in the lungs declines below typical sea level values, haemoglobin still has a high affinity for O2 and remains almost fully saturated. Even though PO2 differs by 20 mmHg there is almost no difference in haemoglobin saturation.
Significance of Steep Portion • PO2reductions below 40 mm Hg produce a rapid decrease in the amount of O2 bound to hemoglobin. • When the PO2 falls below 40 mm Hg, the quantity of O2 delivered to the tissue cells may be significantly reduced. • As PO2decrease in this steep area of the curve, the O2 is unloaded to peripheral tissue as hemoglobin’s affinity for O2 diminishes. • Therefore, small changes in PO2 will release large amounts of O2 from hemoglobin. • * This is critical during exercise when O2 consumption is high.
Factors that affect the O2Dissociation • pH - Change in the blood pH • Temperature- temp increases = the curve moves to the right • Carbon Dioxide – increased PCO2
Example • During exercise, the oxyhemoglobin dissociation curve will shift to the RIGHT • This is because the pH in the body is decreased (from increased lactic acid) AND • Temperature increases during exercise
O2 Transport in muscle • Myoglobin: - Protein that binds with O2 - Found in Skeletal and Cardiac muscle fibers (not in blood) - Acts as a shuttle to transport O2 from muscle cell membrane to the mitochondria - Found in large quantities in slow-twitch fibers (high aerobic capacity) - Smaller amounts in intermediate fibers - Limited quantity in fast twitch fibers
Myoglobin has a similar structure to hemoglobin, but is ¼ weight • Difference in structure = difference in affinity for O2 • Myoglobin has a greater affinity for O2: Therefore the myoglobin-O2 dissociation curve is much steeper = myoglobin releases O2 at very low PO2 values • NB because PO2 in mitochondria of contracting skeletal muscle can be as low as 1mmHg.
Myoglobin stores O2 = reserve O2 for transition from rest to exercise • At the start of exercise there is a lag time from the onset of muscular contraction and increased O2 delivery to the muscles • Therefore O2 bound to myoglobin before exercise acts as a buffer so that muscles can receive O2 until the cardiopulmonary system can meet the new O2 demand
At the end of exercise:- myoglobin- O2 stores must be replenished to ensure O2 is available for the next time exercise begins • Therefore O2 consumption above rest contributes to the O2 debt • i.e. O2 consumption continues after exercise has stopped leading to an O2 debt (O2 deficit) (Anaerobic metabolism of lactate – also called EPOC Post Exercise Oxygen Consumption)
Carbon Dioxide Transport in Blood • CO2 transported in the blood by:1. Dissolved CO2 (±10%)2. CO2 bound to hemoglobin (±20%)3. Bicarbonate (HCO3¯)(±70%)
CO2 is converted to bicarbonate in red blood cells: • A high PCO2 causes CO2 to combine with water, forming carbonic acid. • This reaction is rapidly catalyzed by the enzyme Carbonic Anhydrase • The carbonic acid then dissociates into bicarbonate ion and hydrogen ion. • The hydrogen ion then binds with hemoglobin • The bicarbonate ion diffuses out of the red blood cell into the blood plasma
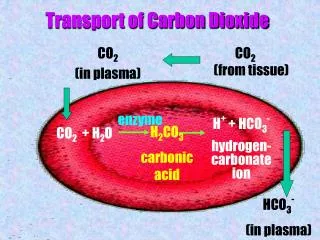
Carbon Dioxide Transport Transport of CO2 CA CO2 + H2O H2CO3 Carbonic Acid H2CO3 H+ + H-CO3 Bicarbonate ion
Bicarbonate Ion Exchange • Because bicarbonate carries a negative charge (anion), removal of a negatively charged molecule from a cell = electrochemical imbalance • Therefore the negative charge must be replaced • Bicarbonate is replaced by chloride (Cl¯) which diffuses from the plasma into the red blood cell • This is called chloride shift the shift of anions into red blood cells as blood moves through tissue capillaries
When blood reaches the pulmonary capillaries:PCO2 of the blood is greater than that of the alveolus = CO2 diffuses out of the blood across the blood-gas interface • At the lungs:Binding of O2 to hemoglobin causes a release of the hydrogen ions (which are bound to hemoglobin) to promote the formation of carbonic acid • H+ + HCO3¯ H2CO3
In conditions where PCO2 is low (at the alveolus), carbonic acid then dissociates into CO2 and H2O H2CO3 CO2 +H2O • The release of CO2 from the blood into the alveoli is removed from the body in expired gas (CO2 we breathe out)
Revision Questions • 1. What is the amount of hemoglobin found in a normal male and female? (2) • 2. What is the amount of oxygen carried in a normal male and female? (2) • 3. What is partial pressure? (2) • 4. Explain the oxghemoglobin dissociation curve, focusing on the use, flat and steep portions (10) • 5. What factors affect the oxghemoglobin dissociation curve? (3)
Revision Questions • 6. How does exercise affect the oxghemoglobin dissociation curve? (3) • 7. What is myoglobin and where is it found? (4) • 8. How is myoglobin different to hemoglobin? (4) • 9. What are the differences in myoglobin and oxygen at the start and end of exercise? Why does this happen? (8) • 10. What are the way in which carbon dioxide is transported? (3) • 11. How is carbon dioxide converted to bicarbonate? (5) • 12. Explain bicarbonate exchange. (8)