“SUPPORT” PRESENTATION 08-19-13 Joel E Frader, MD, MA
200 likes | 362 Vues
“SUPPORT” PRESENTATION 08-19-13 Joel E Frader, MD, MA Medical Director, Bridges Palliative Care Program, Lurie Children’s Hospital A Todd Davis Professor of Academic General Pediatrics Professor of Medical Humanities and Bioethics Feinberg School of Medicine, Northwestern University

“SUPPORT” PRESENTATION 08-19-13 Joel E Frader, MD, MA
E N D
Presentation Transcript
“SUPPORT” PRESENTATION 08-19-13 Joel E Frader, MD, MA Medical Director, Bridges Palliative Care Program, Lurie Children’s Hospital A Todd Davis Professor of Academic General Pediatrics Professor of Medical Humanities and Bioethics Feinberg School of Medicine, Northwestern University Kelly Michelson, MD, MPH Attending Physician, Ann & Robert H. Lurie Children's Hospital of Chicago Associate Professor of Pediatrics and the Buehler Center on Aging, Health & Society, Northwestern University Feinberg School of Medicine William J. Muller, MD, PhD Assistant Professor, Pediatrics, Northwestern University Feinberg School of Medicine Fellowship Program Director, Pediatric Infectious Diseases Attending Physician, Ann & Robert H. Lurie Children’s Hospital of Chicago
Surfactant, Positive Pressure, and Oxygenation Randomized Trial in Extremely Low Birth Weight Infants (SUPPORT trial) Lurie Children’s IRB August 19, 2013 William J. Muller, MD, PhD
ELBW premature infants are at risk for multiple medical issues • Respiratory distress syndrome / Chronic lung disease • Retinopathy of prematurity • Mortality • Goals of the study • Does positive airway pressure during resuscitation after birth help decrease the severity of lung disease in premature babies? • At the time the study began (2005) there were no recommendations regarding the use of CPAP/PEEP in the delivery room/nursery for premature infants • Some prior studies suggested CPAP/PEEP could decrease the requirement for mechanical ventilation, decrease the need for supplemental oxygen, and decrease the need for surfactant SUPPORT trial – introduction (1)
ELBW premature infants are at risk for multiple medical issues • Respiratory distress syndrome / Chronic lung disease • Retinopathy of prematurity • Mortality • Goals of the study • Can controlling oxygen saturation at the lower end of the standard of care decrease retinopathy of prematurity? • At the time the study began recommendations were to provide supplemental oxygen to keep saturation between 85-95% • Retinopathy of prematurity was known to be associated with prolonged use of supplemental oxygen • It was not known whether keeping SO2 in the lower end of the recommended range would decrease the risk SUPPORT trial – introduction (2)
Multicenter, randomized controlled trial including hospitals in the NICHD Neonatal Research Network • Parents were asked for consent prior to delivery of babies at risk for birth before gestational age 28 weeks • Babies GA 24 – 27.6 weeks were randomized to early CPAP/PEEP in the delivery room vs. early mechanical ventilation with surfactant • Both methods of management were practiced at the time the study began • Babies in the early CPAP group with signs of respiratory failure would be intubated; if they were <48 hours old they would receive surfactant • Babies in the early surfactant and ventilation group would receive surfactant in the 1st hour of life; for the first 14 days of life, guidelines determined when they would be placed on or taken off CPAP/PEEP or mechanical ventilation SUPPORT trial – study design (1)
Babies were also randomized to target oxygen saturation of 85-89% vs. 91-95% (c/w recommendations at the time) • Patients were in the ventilation arm of the study (CPAP/PEEP vs. surfactant) for the first 14 days of life, and were followed to 18-22 months of age for outcome measures: • Primary outcome: death before discharge or severe retinopathy • Retinopathy defined by prespecified criteria • Original study protocol specified a primary outcome of death before 36 weeks of postmenstrual age, but this was changed to death before discharge before any data analyses were performed • All other outcomes reported were prespecified • Assessment of the need for oxygen at 36 weeks of postmenstrual age • Safety outcomes SUPPORT trial – study design (2)
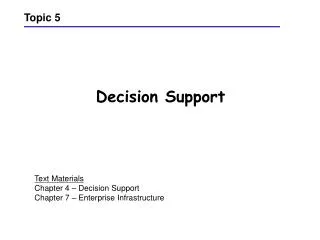
Screening, Randomization, and Primary Outcome. SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network. N Engl J Med 2010;362:1959-1969.
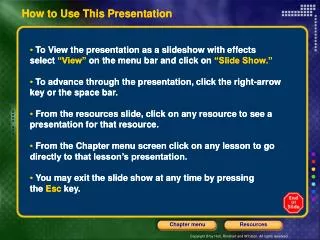
Kaplan–Meier Estimate of Survival to Hospital Discharge, Transfer, or 1 Year of Life. SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network. N Engl J Med 2010;362:1959-1969.
In 2011 the federal Office for Human Research Protections began an investigation into the informed consent process used for this study • On March 7, 2013, a letter to the lead center (University of Alabama-Birmingham) concluded: • “It was alleged, and we determine, that the IRB [institutional review board] approved informed consent documents for this study failed to include or adequately address the following basic element required by HHS [Health and Human Services] regulations at 45 CFR 46.116(a): Section 46.116(a)(2): A description of any reasonably foreseeable risks and discomforts.” SUPPORT trial – controversy
Where to Find the Right SUPPORT When You Really Need It Joel E. Frader, MD, MA A Todd Davis Professor of Academic General Pediatrics Ann & Robert H. Lurie Children’s Hospital of Chicago
Intent of SUPPORT Trial • Focus of much of neonatology (much like peds oncology) • Minimize unintended negative consequences of life-saving interventions • In NIH-funded SUPPORT, one aim: reduce injury from oxygen therapy in premies (24-27 weeks) • Too much O2 vascular proliferation in retina (ROP) • Too little O2 hypoxic/ischemic brain injury (CP, cognitive impairment) • Too much O2 ? Free radical formation, brain injury, ? Other organ damage/death
SUPPORT Design • Two parts: CPAP and safest range of oxygen saturations • CPAP subpart not ethically controversial • Low(er) vs. high(er) saturations subpart generated uproar • Inadequacy of informed consent (documents) • Risk of death from research participation • Lack of disclosure of masking of “true” saturation from clinicians (MDs, RNs, RTs) • This trial unexpectedly showed statistically significant higher death rate in low saturation group • Investigators had worried that high saturations might have association with increased mortality because of free radical organ damage • Low saturation group also had less ROP
After 2010 NEJM Results Report • “Whistleblower” report to OHRP: inadequate IC • March, 2013: OHRP issued determination letter to lead institution (UAB) • Consent form(s) violated federal regulations re: adequacy of research risk disclosure • Requested UAB plan for corrective action • Public Citizen began campaign for OHRP to go further • Investigators, some pediatricians/ethicists protested • NIH Director, NICHD Director, and NIH Policy Director objected • NEJM published ethicists’ letter and NIH bigwig response in same issue (6/5/2013) • Both said OHRP over-reached • Full disclosure: Frader signatory to NEJM letter
Uproar Continues • Public Citizen leaders publish several rejoinders in BMJ • Second group of ethicists countered first group in NEJM (8/10/2013) • Felt OHRP was doing its (required) duty • Other groups generally wary of research with human subjects have chimed in with “we told you so” admonitions • “The People” can’t trust researchers
? Facts • About half the consent forms in the 20+ participating institutions in North America did not mention risk of research-related death • Very few of the consent forms explained the pulse oximetry read-out alterations • We have NO INFORMATION about what was or was not said to parent(s) about risks or research methods • A consent form for a very similar trial (BOOST) in New Zealand clearly explains both possible death and oximetry masking • Similar trials in NZ, Australia, and Europe have not shown increased death rates in subjects treated using lower saturation range
Ethical Claims • Defendants of nondisclosure say: • No research-related risk existed • Trial simply compared two commonly employed (in clinical practice in various NICUs around the world) approaches to maintain saturations • As alterations in pulse oximeters DID correctly alarm when babies’ saturations fell above or below the entire range acceptable in the study, parents did not need to know that detail of the study’s methods • Dissenters say: • The simple fact of randomization, RATHER THAN provision of individualized care, imposes research-related risks, including increased risk of death • Omitting the details of oximeter alteration violates parents’ “right” to know and constitutes deception
What to Make of It All? • At some level, debate is silly • Research over decades has demonstrated inadequacy and irrelevance of consent forms (for clinical care and research) • Real consent involves a (complex) process • Investigators AND regulators should worry about how best to convey information to patients/families in ways pts/families find most helpful • We need more work to develop consensus about level of consent necessary for “comparative effectiveness” or “QI” research examining outcomes when clinicians employ variations on currently accepted therapies • The NZ experience clearly demonstrated decent consent forms can succinctly convey complex info and not undermine study participation (though forms probably irrelevant)
What to Study; What to Say? • New approach to clinical research: community participation • Moves away from what researchers want to know and moves toward defining what’s important to patients/families • E.g., parents of very premature infants may not care much about small trade-offs in impaired vision vs. slightly different death rates. • They may be more concerned with overall happiness, quality-of-life, cognitive function in surviving children • Involves (potential) patients/families in ALL aspects of research design, including aims, methods, consent process, analyzing data, reporting results, etc. • Parents could have helped investigators find out what families of potential subjects want to know about such research participation and how they want to learn about it before granting permission (or not) for enrollment
Final Word • Assumption that individualized clinical care improves outcomes does not hold much water • Numerous historical examples of clinicians pursuing treatments they believe most beneficial but turn out to be without value or harmful • Internal mammary artery ligation for angina/CAD • Gastric freezing for peptic ulcers • ? Propranolol pre-operatively for patients with CAD • Aspirin for children with influenza • Well intentioned docs may not know what’s best, no matter what they believe. • That’s a good (enough) reason to do studies • OHRP can—and has—backed off…