Download
1 / 15
160 likes | 373 Vues
The Effect of Hospitals’ Post-Acute Care Ownership on Medicare Post-Acute Care Use. 1. Department of Family and Community Medicine, University of Missouri-Columbia 2. Division of Health Services Research and Policy, University of Minnesota

E N D
The Effect of Hospitals’Post-Acute Care Ownership on Medicare Post-Acute Care Use 1. Department of Family and Community Medicine, University of Missouri-Columbia 2. Division of Health Services Research and Policy, University of Minnesota 3. Office of Medical Research/Biostatistics, University of Missouri-Columbia Wen-Chieh Lin, PhD 1 Robert L. Kane, MD 2 David R. Mehr, MD, MS 1 Richard W. Madsen, PhD 3 Greg F. Petroski, PhD 3 Funding Sources: Agency for Healthcare Research and Quality
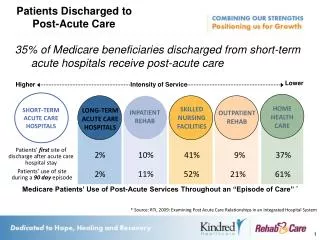
Post-Acute Care (PAC) • Replace a portion of hospital care • Hospitals discharge patients as soon as medically possible • Hospitals minimize resources used through shortened length of stay • Medicare PAC payment system reforms • New financial incentives for PAC settings, but not to hospitals directly • More influential on hospitals owning PAC settings
Study Objectives • To examine the association between PAC use and hospitals’ PAC ownership • To examine the relationship between PAC use and changes in hospitals’ PAC ownership, i.e., added or discontinued PAC ownership, between 1996 and 2000 (pre- and post- payment reforms on HHAs and SNFs)
Data • 5% Medicare beneficiary sample in year 2000 • 6 disease groups with the most frequent PAC utilization • Rehabilitative conditions • Stroke, hip and knee procedures, and hip fracture • Medical conditions • Chronic obstructive pulmonary disease (COPD), pneumonia, and congestive heart failure (CHF)
Statistical Analysis • Multinomial logit regression • Dependent variable: immediate type of PAC service used after hospital discharge • SNF, IRF, HHA, and No Service (reference) • Independent variables • Patient characteristics • Hospital characteristics • Market area characteristics
Hospitals’ PAC Ownership • Own rehabilitation unit • a hospital has a PPS exempt rehabilitation unit • Own SNF • related hospitals for SNFs indicating hospital-based • Own swing bed • a hospital provides swing bed services • Own home care • home care services are provided by staff
The Association between PAC Use and Hospitals’ PAC Ownership
The Association between PAC Use and Hospitals’ PAC Ownership (Contd.)
Changes in Hospitals’ PAC Ownership • Comparing the status of a hospital’s PAC ownership between 1996 and 2000 (pre- and post- payment reforms on HHAs and SNFs) • Yes in 1996 and Yes in 2000 • No in 1996 and Yes in 2000 • Yes in 1996 and No in 2000 • No in 1996 and No in 2000 (reference category)
The Association between PAC Use and Changes in Hospitals’ PAC Ownership
The Association between PAC Use and Changes in Hospitals’ PAC Ownership
Conclusions • The link between PAC use and hospitals’ PAC ownership remained significant in the post-BBA era • A hospital’s PAC ownership was associated with an increased use in this PAC modality, while the likelihood of using other PAC modalities decreased • Substitution between PAC modalities is also driven by hospitals’ PAC ownership
Limitations • Data cover only the initial period (1996 to 2000) of the BBA changes on PAC services • October 2000: HHA prospective payment system • January 2002: IRF prospective payment system • Analyses did not include the partnership and contractual relationship between hospitals and PAC settings
Discussion • Discharging patients to hospitals’ own PAC setting • Improve information sharing • Reduce adverse outcomes during the transition • Unknown whether outcomes are comparable in alternative settings • Implications of outcomes and costs of substitution between PAC settings