Download
1 / 55
570 likes | 1.11k Vues
Acute and Post-Acute Care of the Elderly: Models for Improving Outcomes. Adrienne Green, M.D. Assistant Clinical Professor and Hospitalist University of California San Francisco. Objectives. Review the impact of hospitalization and SNF placement on outcomes in the elderly.

E N D
Acute and Post-Acute Care of the Elderly:Models for Improving Outcomes Adrienne Green, M.D. Assistant Clinical Professor and Hospitalist University of California San Francisco
Objectives • Review the impact of hospitalization and SNF placement on outcomes in the elderly. • Review significance of and risk factors for functional decline in the hospitalized geriatric patient. • Review interventions to prevent functional decline and improve outcomes.
Objectives • Review interventions designed to prevent readmission. • Review needs for improving discharge planning and transitional care for the hospitalized geriatric patient. • Emphasize importance of teamwork in the care of the geriatric patient!
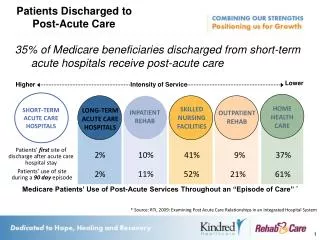
Hospitalization in the ElderlyBackground • Patients >65 40% acute hospitalizations • Current reimbursement demands “quicker and sicker” discharges • Poor outcomes • High 1 year mortality • 30% functional decline • High readmission rates • High rates of home health use • High rates of SNF placement
Prognostic Index for 1-year Mortality in Older Adults after Hospitalization Walter et al. JAMA 2001 • Data • age >70, medical admission • Derivation 1600 pts, university hospital • Validation 1500 pts, community hospital • Demographic, functional, medical factors • Outcome- mortality at 1 year after d/c
Prognostic Index for 1-year Mortality in Older Adults after Hospitalization Walter et al. JAMA 2001 • Independent RF’s for 1 yr mortality • Male • CHF, CA as comorbidities • Functional decline in any ADL at d/c • Cr >3, alb< 3.4
Prognostic Index for 1-year Mortality in Older Adults after Hospitalization Walter et al. JAMA 2001
SNF Outcomes • 20-40% elderly in SNF at some point • 25% annual mortality rate • 50% admitted for short term post-acute care • Outcomes highly dependent on function at admission
Outcomes of Nursing Home CareLewis et al. Gerontologist 1985, AJPH 1985. • 563 pts discharged from 24 NHs Southern CA • 80% admitted from hospital • Cognitive status, functional status, continence predictive of outcome
Case #1 • Mrs. Dee Cline is an 80 y/o woman with a history of asthma admitted to the medical service with community acquired pneumonia and an asthma exacerbation. She is treated with antibiotics, bronchodilators and prednisone with improvement in her respiratory status over the next 4 days.
Case #1 • Prior to admission the patient lived alone and used a cane for ambulating. She was independent in all ADL’s but required help with some IADl’s including shopping, laundry, cooking and cleaning. Mrs. C has some close friends but no family nearby.
Case #1 On the planned day of discharge, Mrs. C tells the nurse that she is having difficulty getting up from the chair and that she feels “very shaky” while walking. Discharge is delayed even though the patient is otherwise stable from a medical standpoint.
Functional Decline • Decreased ability to perform ADL’s • Deteriorization in self care skills
Functional DeclineQuestions • What percentage of geriatric patients suffers functional decline during hospitalization? • 30% • What percentage of these patients returns to their prior baseline function? • 50%
Functional Outcomes in Medical Illness and Hospitalization in Older PersonsSager et al. Arch Int Med. 1996. • Prospective analysis of 1300 pts HOPE trial • medical diagnoses • Independence in 6 ADLs and 7 IADLs • 2 weeks PTA • discharge • 3 months post discharge
Functional Outcomes in Medical Illness and Hospitalization in Older PersonsSager et al. Arch Int Med. 1996.
Functional Outcomes in Medical Illness and Hospitalization in Older PersonsSager et al. Arch Int Med. 1996.
Functional DeclineQuestions • Does functional decline effect patient outcomes and prognosis? • Mortality (increases with # of ADL deficits) • SNF placement • LOS • Readmission • Impact on independence, quality of life • Costly
Questions • What is the etiology of functional decline in the hospitalized geriatric patient?
“Cascade to Dependency” Creditor. Ann Int Med. 1993.
“The Dysfunctional Syndrome” Functional Older Person Acute Illness/Possible Dysfunction Hospitalization Hostile Environment Depersonalization Bedrest Starvation Medicines Procedures Depressed Mood Physical Impairment Dysfunctional Older Person Palmer et al. Clin Ger Med 1998
Functional DeclineQuestions • At what point could the healthcare team have identified Mrs. C’s risk of functional decline? • On admission • What are her specific risk factors? • Age, IADL dependency on admission
Hospital Admission Risk ProfileSager et al. JAGS 1996. • Prospective cohort study, subgroup of HOPE, age >70, medical admits • Scoring System
Risk Profile • Practical and simple • No additional training • Little extra time • Can be performed by M.D., R.N., Case manager, Social Worker….
Questions • Are there effective models for the prevention of functional decline (and other poor outcomes) for the hospitalized geriatric patient?
Functional DeclineInterventions • Geriatric consultation • Acute Care of Elder units (ACE) • Hospital Elder Life Program (HELP) • Nurses Improving Care for Health System Elders (NICHE)
Medical Unit to Improve Functional Outcomes (ACE)Landefeld et al. NEJM. 1995. • Prepared environment • Carpets, handrails, large clocks • Patient centered care by a multidisciplinary team • Daily eval with protocols to address self care, nutrition, mobility, cognitive status, skin… • Daily rounds by team
Medical Unit to Improve Functional OutcomesLandefeld et al. NEJM. 1995. • Discharge planning • Started by SW on day of admission • Medical care review • Geriatrician and geriatric NP to review care, make recommendations, provide supervision
Much better Better Unchanged Worse Much worse Usual care 13% 11% 54% 13% 8% ACE 21% 13% 50% 7% 9% Medical Unit to Improve Functional OutcomesLandefeld et al. NEJM. 1995. • Randomized trial, univ hospital 300 medical pts each to ACE unit vs. usual care Functional Status Admit to Discharge
Medical Unit to Improve Functional OutcomesLandefeld et al. NEJM. 1995. Counsell et al. JAGS. 2000. • No difference in functional outcomes at 3 months. • No difference in readmission rate. • ACE in a community hospital • No difference in functional outcomes • Improved process of care • Improved pt, family and provider satisfaction
ACE Units- getting started • 100 in U.S. • Resources • Summa Foundation (Akron, OH) • Initial $$ with overall savings for hospital over time
The Hospital Elder Life ProgramInouye et al. JAGS 2000. • Goals • Prevent cognitive and physical decline • Promote independence • Assist with transitions • Prevent readmission • Multidisciplinary intervention instituted hospital wide • Prior data for prevention of delirium
The Hospital Elder Life ProgramInouye et al. JAGS 2000. • Patients age >70 and one RF for cognitive or functional decline • MMSE <24 • Any mobility or ADL impairment • Dehydration (BUN/Cr >18) • Vision or hearing impairment
Geriatric nurse specialist Elder life specialist/director Geriatrician Volunteers Rehab services Chaplain Pharmacy Nutrition Psychiatry nurse Social Work Care Coordination The Hospital Elder Life ProgramInouye et al. JAGS 2000.
Daily visits Orientation Sleep enhancement Oral hydration Feeding assistance Therapeutic activities Early mobilization Vision, hearing protocols Geriatric nursing assessment Interdisciplinary rounds Provider education Community links and follow up Geriatric consultation Interdisciplinary Consults- pharmacy, nutrition, chaplain etc. The Hospital Elder Life ProgramInouye et al. JAGS 2000.
The Hospital Elder Life ProgramInouye et al. JAGS 2000. • Outcomes, 1500 pts
HELP- getting started • www.info.med.yale.edu/intmed/elp • HospitalElderLife@yale.edu • Training materials $4000, equipment $3500 to start and $2000/yr • Training manuals, tapes, business, management, clinical tools • $$ for elder life specialist, nurse specialist, volunteer coordinator, provider education
Nurses Improving Care for Healthsystem EldersFulmer et al. Geriatric Nursing 2002. • Models for improving nursing care throughout the hospital • Geriatric Institutional Assessment Profile • Target needs, education, protocol development • Nursing practice protocols • cognitive assessment, eating/feeding, pain management, restraints, falls, pressure ulcers, sleep, incontinence • Geriatric resource nurse model
Nurses Improving Care for Healthsystem EldersFulmer et al. Geriatric Nursing 2002. • SPICES screening tool • Skin impairment • Poor nutrition • Incontinence • Cognitive impairment • Evidence of falls, functional decline • Sleep disturbance
NICHE- getting started • 100 hospitals • NICHE package $7800 • Leadership conference • GIAP data analysis • Practice protocols and models of care • Additional $$ for R.N. training, institutional leadership (geriatric CNS, NP), patient care items • www.hartfordign.org
Case #2 Mr. F is a 75 y/o man with mild dementia, CAD, HTN, and recently diagnosed CHF. He was in good health until 6 weeks PTA when he was admitted with progressive DOE, orthopnea and edema. ECHO demonstrated severe diastolic dysfunction and hypokinesis from old MI. With aggressive diuresis and BP control, Mr. F’s symptoms resolved and he was discharged home on hospital day #3. His PCP was notified to assist with follow up.
Case #2 Mr. F is now readmitted with recurrence of all his symptoms. Clinically he appears to have a CHF exacerbation that is felt to be due to medication and dietary non-compliance. Mr. F lives alone but has 2 daughters nearby. He is able to perform his own ADLs but requires assistance with IADLs. He has been reluctant to accept help in the home.
Case #2 Mr. F again responds to diuresis and BP management. On hospital day #4, he is told he can go home. Later that morning his physician receives an irate phone call from his daughter. She is surprised by the discharge plan, very anxious about potential for yet another rehospitalization and states that she doesn’t think her father can manage on his own any longer. She demands a meeting with the physician and social worker later in the day.
Case #2 Discharge is delayed even though the patient is stable from a medical standpoint. What went wrong?
Questions What could have been done to prevent this uncomfortable confrontation? Are there effective models for optimizing the transition of elderly patients from the acute to post-acute setting?
Transitional Care and Discharge PlanningNaylor. Ann Rev Nurs Res. 2002. • Transitional Care • Bridge gaps between providers, services, sites of care • Promote safe and timely transfer of pts from one level of care to another • Provide accurate and complete communication between providers and sites of care
Transitional Care and Discharge PlanningNaylor. Ann Rev Nurs Res. 2002. • Patients and families • 1/3 pts unmet needs after discharge • Lack of input into discharge decisions • Lack of knowledge, education • 1/3 with >1 component of d/c plan not implemented • ½-¾ recommended info not transmitted to SNFs and home health