Nutrition – Use and indications
130 likes | 255 Vues
Nutrition – Use and indications. Malnutrition leads to poor wound healing, post-operative complications and sepsis. Adequate nutritional support is important for critically ill patients and should be provided early during the illness.

Nutrition – Use and indications
E N D
Presentation Transcript
Nutrition – Use and indications • Malnutrition leads to poor wound healing, post-operative complications and sepsis. • Adequate nutritional support is important for critically ill patients and should be provided early during the illness. • Evidence for improved outcome from early nutritional support exists for patients with trauma and burns. • Enteral nutrition is indicated when swallowing is inadequate or impossible but gastrointestinal function is otherwise intact. • Parenteral nutrition is indicated where the gastrointestinal tract cannot be used to provide adequate nutritional support, e.g. obstruction, ileus, high small bowel fistula or malabsorption. • Parenteral nutrition may be used to supplement enteral nutrition where gastrointestinal function allows partial nautritional support.
Consequences of malnutrition Underfeeding Overfeeding Loss of muscle mass Increased VO2 Reduced respiratory function Increased VCO2 Reduced immune function Hyperglycaemia Poor wound healing Fatty infiltration of liver Gut mucosal atrophy Reduced protein synthesis
Calorie requirement • Various formulae exist to calculate the patient’s basal metabolic rate but they are often misleading in critical illness. • Metabolic rate can be measured at the bedside by indirect calorimetry but most patients will require 2000-2700 Cal/day or less if starved or underweight.
Nitrogen requirements • Nitrogen excretion can be calculated in the absence of renal failure according to the 24th urea excretion. Nitrogen (g/24h) = 2 + Urinary urea (mmol/24h) x 0.028 • However, as with most formulae, this method lacks accuracy. • Most patients require 7-14g/day.
Other requirements • The normal requirements of substrates, vitamins and trace elements are tabled opposite. • Most critically ill patients require folic acid and vitamin supplementation during nutritional support, e.g. Solvitio. • Trace elements are usually supplemented in parenteral formulae but should not be required during enteral nutrition.
Normal daily requirements (for a 70kg adult) Water 2100ml Trace elements Energy 2000-2700Cal Iron 1-2mg Nitrogen 7-14g Copper 0.5-1.0mg Glucose 210g Managanese 1-2ug Lipid 140g Zinc 2-4mg Sodium 70-140 mmol Iodide 70-140 ug Potassium 50-120 mmol Flurodie 1-2mg Calcium 5-10 mmol Magnesium 5-10 mmol Phosphate 10-20 mmol Vitamins Thiamine 16-19mg Riboflavin 3-8mg Niacin 33-34mg Pyridoxine 5-10mg Folate 0.3-0.5mg Vitamin C 250-450mg Vitamin A 2800-3300iu Vitamin D 280-330iu Vitamin E 1.4-1.7iu Vitamin K 0.7mg
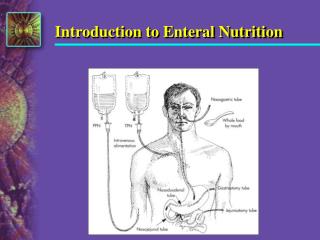
Enteral nutrituion • Routes include naso-gastric, naso-duodenal, gastrostomy and jejunostomy. • Nasal tube feeding should be via a soft fine born tube to aid pateint comfort and avoid ulceration of the nose or oesophagus. • Prolonged enteral feeding may be accomplished via a percutaneous gastrostomy. • Enteral feeding provides a more complete diet than parenteral nutrition, maintains structural integrity of the gut, improves bowel adaptation after resection and reduces infection risk.
Feed Composition • Most patients tolerate an iso-osmolar, non-lactose feed. Carbohydrates are provided as sucrose or glucose polymers (other than lactose). • Protein may be as whole protein or oligopeptides. There is evidence that oligopeptides are better absorbed than free amino acids in ‘elemental’ feeds. • Fats may be provided as medium chain or long chain triglycerides. • Medium chain triglycerides are better absorbed. A standard feed will be formulated at 1Cal/ml. • Special fees are available for special purposes, e.g. high protein, fat or carbohydrate requirements, restricted salt, concentrated (1.5 or 2Cal/ml) for fluid restriction, or glutamine enriched. • Impact is a formula supplemented with arginine, nucleotides and fish oil; it may reduce hospital stay and infectious complications in critically ill patients.
Complications • Tube placement : tracheobronchial intubation, nasopharyngeal perforation, intracranial penetration (basal skull fracture), oesophageal perforation • Reflux • Pulmonary aspiration • Nausea and vomiting • Diarrhoea : large volume, bolus feeding, high osmolality, infection, lactose intolerance, antibiotic therapy, high fat content • Constipation • Metabolic : dehydration, hyperglycaemia, electrolyte imbalance
Parenteral nutrition Feed composition • Carbohydrate is normally provided in the form of concentrated glucose. While it is possible to provide the body’s energy requirements with glucose alone, it si advantageous to provide 30-40% of total calories as lipid (i.g. soya bean emulsion). • The nitrogen source should contain appropriate quantities of all essential and most of the non-essential amino acids. • There should be a high branched chain amino acid content and a high concentration of glycine should be avoided. • Carbohydrate, lipid and nitrogen sources are usually mixed into a large bag in a sterile pharmayc unit. Vitamins, trace leements and appropriate electrolyte concentration can be achieved ina single infusion, thus avoiding multiple connections.
Choice of parenteral feeding route Central venous • A dedicated central venous catheter (or lumen of a multi-lumen catheter) is placed under sterile conditions. A subcutaneous tunnel is often used to separate the skin and vein entry sites. • This probably reduces the risk of infection and certainly identifies the special purpose of the catheter. • It is important that blood samples are not taken and other injections or infusions are not given through the feeding lumen. • The main advantage of the central venous route is that it allows infusion of hperosmolar solution, providing adequate energy intake in reduced volume.
Peripheral venous • Parenteral nutrition via the peripheral route requires a solution with osmolality <800mOsm kg. • Either the volume mus be increased or the energy content (particularly from carbohydrate) reduced. • Peripheral cannulae sites must be changed frequently
Complications • Catheter related misplacement infection Thromboembolism • Fluid excess • Hyperosmolar hyperglycaemic state • Electrolyte imbalance • Hypophosphataemia • Metabolic acidosis Hyperchloraemia Metabolism of cationic amino acids • Rebound hypoglycaemia high endogenous insulin levels • Vitamin deficiency folate : pancytopenia thiamine : encephalopathy vitamin K : hypoprothrombinaemia • Vitamin excess vitamin A: dermatitis vitamin D: hypercalcaemia • Fatty liver