Download
1 / 32
320 likes | 347 Vues
Explore the impacts of rising uninsured rates and Medicaid on safety-net hospitals through NHAMCS data analysis. Learn about ED burden factors and health disparities.

E N D
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for Health Statistics Characteristics of EDs serving high volumes of safety-net populations Catharine W. Burt , Ed.D. Chief, Ambulatory Care Statistics Branch July 13, 2004 Data Users Conference
Topics • Why do we care? • What is the NHAMCS? • What other data sources were used? • What are the findings? • So what?
“ Rising numbers of uninsured Americans, an increasing price-driven health care marketplace, and rapid growth in enrollment of Medicaid beneficiaries in managed care plans may have critical implications for the future viability of American’s health care safety net that serves a large portion of low-income and uninsured Americans.” America’s Health Care Safety Net ...Institute of Medicine, 2000
What is the health care safety net? • Emergency departments • Public hospital systems • Community health centers • Rural health clinics • Other clinics run by local health departments
What are the vulnerable populations? • Uninsured persons • Low income, under-insured persons • Medicaid beneficiaries • SCHIP beneficiaries • Persons with special health care needs
Why are safety-net hospitals so concerned? • Provide large amount of uncompensated care • Increased Medicaid managed care increases their risk of under-compensation • Decreased revenue from Medicare and private insurance • Decreased Medicaid Disproportionate Share Hospital (DSH) payments from States • Many hospitals and EDs closed
What are DSH payments? • Federal matching to State giving • History of creative funding • 1997 BBA reduced size of DSH payments • 2000 BIPA modified the DSH criteria • MIUR > +1 sd in state • > 1% MIUR (optional) • >25% LIUR
Current study goals • Use NHAMCS ED data to identify high-burden EDs. • Use NHAMCS ED visit data, hospital information, and community factors to describe high-burden EDs in comparison to low-burden EDs. • Describe which factors are most associated with high burden.
National Hospital Ambulatory Medical Care Survey (NHAMCS) • Conducted annually since 1992 • Endorsed by emergency medicine associations • Census Bureau — personal interview w/ medical record abstraction: 93% response • Complex sample of 600 non-Federal, general & short stay hospitals Patient and visit characteristics for 25,611 ED encounters in 2000 • Hospital characteristics for 376 EDs
Other data sources • HRSA’s Area Resource File • State and county level data • CMS’s Medicaid DSH payments for 2000
High safety-net ED definition • If the ED met one or more of the following criteria • >30% Medicaid patient visits • >30% uninsured patient visits • >40% combined Medicaid and uninsured
High Medicaid/low uninsured High Uninsured/low Medicaid High both High combined Not Safety net Distribution of hospital EDs by safety-net criteria: United States, 2000 9.4 7.7 2.1 17.0 63.9 1 10 100 Percent of hospital EDs
Distribution of hospital EDs by percent combined Medicaid & uninsured visits grouped by safety-net criteria: United States, 2000 Percent of visits 90+ 85-89 80-84 75-79 70-74 65-69 Met 2+ criteria for safety net 60-64 Met 1 criteria for safety net 55-59 Met no criteria for safety net 50-54 45-49 40-44 35-39 30-34 25-29 20-24 15-19 10-14 5-9 1-4 0 0 2 4 6 8 10 12 14 Percent of hospital EDs
Domains of ED characteristics studied • Hospital • Community • Patient mix • Diagnosis mix (Billings’ ACS algorithm) • Visit severity, content, and outcome
Located in the South Any Medicaid DSH payment Medicaid DSH amount Annual ED volume Public owned Medical school affiliation Located in a non-metro area Hospital: -0.1 0.1 0.2 0.3 0.4 0.5 0 Correlation coefficient
Probability that an ED has high safety-net burden by geographic region Midwest .16 Northeast .25 West .24 South .61 SOURCE: CDC/NCHS
Distribution of EDs by geographic region according to safety-net status Northeast Midwest South West South 23% Low safety net South 65% High safety net 0% 20% 40% 60% 80% 100% Percent of EDs
Percent in poverty Unemployment rate State's DSH payment ratio ED visit rate HMO penetration rate Income per capita Primary care docs per pop Percent age 65+ Community: -0.4 -0.2 0 0.2 0.4 0.6 Correlation coefficient
% Medicaid % Uninsured % Black or African American % Child % Medicaid risk plan % Medicare % Senior Patient Mix: -0.6 -0.4 -0.2 0 0.2 0.4 0.6 0.8 Correlation coefficient
% nonurgent % emergent, primary care treatable % mental health % unclassified % alcohol % injury % emergent, avoidable % emergent, not avoidable Diagnosis mix: -0.3 -0.2 -0.1 0 0.1 0.2 0.3 0.4 Correlation coefficient
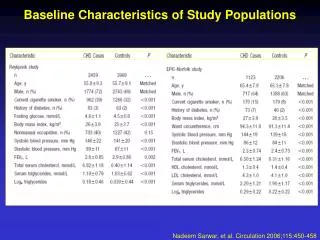
Nonurgent * Emergent, PC treatable * Emergent, avoidable Emergent, unavoidable * Injury * Mental health Other diagnosis Comparison of diagnosis mix using Billings' algorithm by safety-net status Low safety net High safety net 16.9 21.2 19.3 21.3 8.1 7.3 12.4 10.7 32.8 28.1 2 1.9 8.5 9.6 0 5 10 15 20 25 30 35 40 Percent of visits * Difference is significant at p<.05
% of admits that are Medicaid % of admits that are Medicaid % Left before being seen % Left before being seen % of admits that are uninsured % of admits that are uninsured Mean waiting time to see physician Mean waiting time to see physician % Resident/intern seen % Resident/intern seen % Triaged as emergent or urgent % Triaged as emergent or urgent % No follow-up planned % No follow-up planned Mean drug mention rate Mean drug mention rate % of Medicaid patients admitted % of Medicaid patients admitted % Transfer to another facility % Transfer to another facility % arrive via ambulance % arrive via ambulance % of uninsured patients admitted % of uninsured patients admitted % IV fluids administered % IV fluids administered % Admitted to hospital % Admitted to hospital Visit severity, content, and outcome: -0.6 -0.4 -0.2 0 0.2 0.4 Correlation coefficient
Corr w. % Uninsured 0.6 & 0.4 & & & & 0.2 & & & & & & & & & & & & & & & & 0 & & & & & & & & & & & & & & & & -0.2 & & & & & -0.4 Corr w. % Medicaid Plot of bivariate correlation coefficients between ED characteristics and sizes of the Medicaid and uninsured burdens
Co-distribution of linear associations between ED characteristics and size of Medicaid and uninsured burdens Medicaid burden - 0 + ACS % nonurgent % of admits that are uninsured + Located in South Mean waiting time State's DSH payment ratio % left before being seen % black or Afican American ED visit rate % resident/intern % IV fluids Any DSH payment remaining 12 characteristics Income per capita ACS % emergnet, primary care Uninsured burden % injury treatable 0 % arrive via ambulance Unemployment rate % child Percent in poverty % of admits that are Medicaid % senior % Medicare ACS % emergent, avoidable % admit to hospital % transfer % pop 65+ - Located in non-MSA area Primary care doc per pop ACS % emergent, not avoidable Characteristics in the + or - association cells are based on correlation coefficients that are significantly different from zero (p<.01).
Role of DSH payments • 41% of high-burden EDs receive payments compared with 25% of low-burden EDs • State generosity is the highest determinant of whether a hospital receives a DSH payment • State mean as standard puts hospitals in heavy-demand States at risk for no financial supplements
Probability that an ED received a Medicaid DSH payment by safety-net status and region Midwest LSN=.20 HSN=.56 Northeast LSN=.50 HSN=.64 West LSN=.06 HSN=.47 South LSN=.28 HSN=.33 SOURCE: CDC/NCHS
Uninsured Medicaid Rate per 100 persons 25 21.8 20.6 20 15.9 15 13.6 11.7 11.3 10.1 9.2 10 5 0 Northeast Midwest South West Regional variation in rates of uninsured and Medicaid persons under age 65: United States, 1998 SOURCE: A Shared Destiny (IOM 2003)
Uninsured persons Northeast Midwest South West Medicaid enrollees High safety-net EDs 0% 20% 40% 60% 80% 100% Comparison of percent distributions
State Medicaid DSH payment per Medicaid enrollee or uninsured person: United States, 2000 DSH per person $400+ $200-399 $100-199 $50-99 <$50 Missing SOURCE: CDC/NCHS
So what? • One-third of EDs carry a large burden of Medicaid or uninsured care, rarely both. • Hospitals in the southern states are at greatest risk of having high safety-net EDs • DSH payments help but vary widely across Nation. • More Federal funding may be needed to distribute help more widely.