Download

1 / 24
240 likes | 354 Vues
Differences in Access to Care for Asian and White Adults. Merrile Sing, Ph.D. September 8, 2008. Policy Context. Many Asians face significant linguistic and cultural barriers ~ 25% of Asians live in linguistically isolated households (Census 2000) ~ 63% of Asians are immigrants (Census 2000)

E N D
Differences in Access to Care for Asian and White Adults Merrile Sing, Ph.D. September 8, 2008
Policy Context • Many Asians face significant linguistic and cultural barriers ~ 25% of Asians live in linguistically isolated households (Census 2000) ~ 63% of Asians are immigrants (Census 2000) • Some Asian American subgroups are at greater risk than non-Hispanic Whites for certain diseases, such as diabetes, stomach and liver cancer, hepatitis B, and tuberculosis 2
Research Objectives • To estimate adjusted differences in access to care between non-Hispanic White and Asian adults • To identify factors that have the greatest marginal effects on improving access to care 3
Previous Research • Moy et al. (2008). “Community Variation: Disparities in Health Care Quality Between Asian and White Medicare Beneficiaries.” • Miltiades and Wu (2008). “Factors Affecting Physician Visits in Chinese and Chinese Immigrant Samples.” • Snyder et al. (2000). “Access to Medical Care Reported by Asians and Pacific Islanders in a West Coast Physician Group Association” • AHRQ (2007), National Healthcare Disparities Report 4
Study Design • Data are from the Medical Expenditure Panel Survey (MEPS) & Area Resource File, 2002 - 2005 • MEPS contains a nationally representative sample of households in the U.S. civilian, non-institutionalized population • Sample includes non-Hispanic adults age 18 and older • There are 3,779 Asians and 52,498 Whites • Andersen typology of access to care is used • Outcome variables are binary • Usual source of care (excluding emergency room) • At least one office visit during past year 5
Andersen Typology:Control variables Access depends on: • Predisposing characteristics • Enabling Resources • Illness level or perceived need 7
Predisposing Characteristics • Demographic Age, sex, marital status • Social structure Education Acculturation Difficulty speaking English In linguistically isolated family Immigrant < 5 years in U.S. Immigrant 5 – 14 years in U.S. • Attitudes Overcome illness without medical professional More willing to take risk Always uses seat belt 8
Enabling Resources • Family Income Insurance coverage • Community Urban-rural (using Metropolitan Statistical Areas) Census Region (4) Active non-federal MDs/ 1,000 population (county) Number of Federally Qualified Health Centers (county) Percent Asian population in county 9
Illness/Perceived Need • Self-rated general health • Poor mental health (Mental Component Summary) • Number of chronic conditions 10
Methods 11
Estimation Methods • Unadjusted differences in means • Adjusted differences (multivariate logistic regressions) • Marginal effects estimated by method of recycled predictions • Standard errors estimated using balanced repeated replicates 12
Marginal effects onAccess to care Which factors have the greatest marginal effects on improving access to care? • Predisposing conditions with and without acculturation variables • Enabling resources • Perceived need • All control variables 13
Unadjusted Differences 14
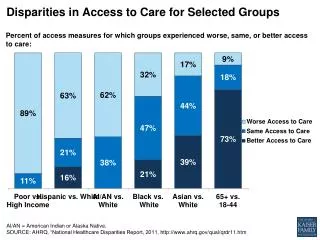
Access to CareAdults Age 18+ ** ** * (**) Significantly different from White at 0.05 (0.01) level or better Source: MEPS 2002 – 2005, adults eligible for access supplement 15
AcculturationImmigrants ** ** ** * (**) Significantly different from White at 0.05 (0.01) level or better Source: MEPS 2002 – 2005, Adults eligible for Access Supplement 16
AcculturationEnglish Language ** ** * (**) Significantly different from White at 0.05 (0.01) level or better Source: MEPS 2002 – 2005, Adults eligible for Access Supplement 17
Variables associated withUsual Source of Care Marginal effect Asian - 0.039* (0.019) EnablingPredisposing Income immigrant < 5 yrs in U.S. Insurance status immigrant 5 - 14 yrs in U.S. MSA Difficulty w/ English Census Region Asian * Difficulty w/English family size Perceived need age number of chronic cond. gender self-rated health marital status attitudes Year 2004 - Year 2005 - Source: MEPS 2002 - 2005 19
Variables associated withOffice Visit(s) Marginal effect Asian - 0.077** (0.015) EnablingPredisposing Income immigrant < 5 yrs in U.S. Insurance status Difficulty w/ English MSA Census Region education Active MDs/ 1000 pop. family size age Perceived need gender number of chronic cond. marital status self-rated general health attitudes self-rated mental health Year 2004 + Source: MEPS 2002 - 2005 20
Marginal Effects on Access to Care Unadjusted Usual Source of Care Office Visit(s) White 0.811 (0.004) 0.784 (0.003) Asian 0.701 (0.013) 0.630 (0.011) Difference -0.110 ** - 0.154 ** Adjusted differences: Marginal effects controlling for: Usual Source of Care Office Visit(s) Predisposing (w/o acculturation) - 0.115 ** - 0.143 ** Predisposing (w/ acculturation) - 0.055 **- 0.102 ** Enabling - 0.078 ** - 0.123 ** Perceived need - 0.068 ** - 0.098 ** All variables - 0.039 ** - 0.077 ** 22
Conclusions • Asian adults were less likely than Whites to have a usual source of care or an office visit, after controlling for predisposing and enabling characteristics and perceived need Greatest Marginal Effects on Access to Care Predisposing Enabling Perceived w/ acculturation Need Usual Source of Care√ Office Visit √ 23
Policy Relevance Findings suggest areas to focus on for improving access to care for Asian adults: • Translating general medical information and Medicaid applications into Asian languages may improve access to care for some Asians • Educating providers about differences in culture and disease incidence for Asians compared with non-Hispanic Whites 24