Chapter 8
Chapter 8. Oral malignant neoplasms & premalignant lesion. I . Oral Malignant Neoplasm. Classification according to the tissue of origin: 1- Squamous cell carcinoma 2- Lymphoepithelioma 3- Basal cell carcinoma 4- Malignant melanoma 5- Sarcomas.

Chapter 8
E N D
Presentation Transcript
Chapter 8 Oral malignant neoplasms & premalignant lesion
I . Oral Malignant Neoplasm Classification according to the tissue of origin: 1- Squamous cell carcinoma 2- Lymphoepithelioma 3- Basal cell carcinoma 4- Malignant melanoma 5- Sarcomas
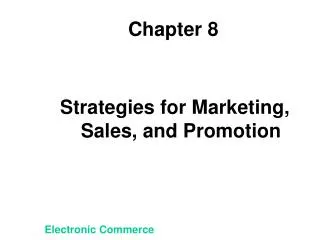
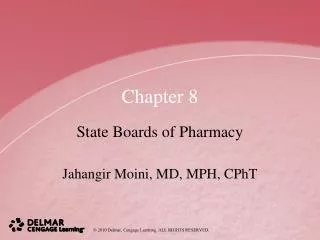
All white & red lesions be submitted for M/E in order to determine their true nature High-risk sites for development of oral carcinoma. The shaded U-shaped area accounts for only about 20% of the whole area of the interior of the mouth but is the site of over 70% of oral cancers.
1- Squamous cell carcinoma - Definition : A common epithelial malignancy of the oral mucosa appearing as red , white , or ulcerated area. SCC is the most common oral cancer. - Etiology : While the cause of oral SCC is not known with certainly , several risk factors have been identified : Tobacco , alcohol , viruses & sunlight . 1) Tobacco : Oral SCC occurs 5-10 times more commonly in cigarette smokers. A number of studies have shown that patients with oral SCC are far more common likely to use tobacco products than the general population. The risk of developing oral SCC 5-10 times in cigarette smokers than in non-smokers .
As might be expected , the risk of cancer development increases with the number of cigarettes consumed each day & the number of years that the habit has been pursued . After cessation of tobacco use the risk of developing oral SCC declines. • Oral SCC is more common in those who use other forms of tobacco . • Unlike lung cancer where cigarette smoking is the primary etiologic culprit , pipe & cigar smoking as well as using chewing tobacco & snuff has be implicated in the cause of oral SCC ,. The heat generated from the stems of pipes has been suggested as causing some lip & palate cancers. • Smokeless tobacco ( chewing tobacco & snuff) is associated with cancers of the buccal mucosa & gingiva. • The use of these of these products is of particular concern because of their use by youngsters as they emulate tobacco – chewing professional baseball players.
2- Alcohol : • Oral SCC is more common in heavy users of alcohol. It has been long recognized that alcohol abuse & development of oral SCC are related . • Here again , several studies have provided the basis for this linkage. . It is postulated that excessive alcohol use dries the oral mucous membrane somehow making it susceptible to cancer development . Like cigarette smoking , the incidence of oral SCC declines with cessation of alcohol use. It has been confirmed in later studies heavy alcohol use is the major risk factor for development of oral SCC. Oral SCC is often found in those who both smoke & drink. • Cigarette & alcohol are , therefore , associated with the development of most oral SCCs . It is a common observation that heavy alcohol users are also heavy smokers. The two combined are a powerful risk factor for development of this disease.
3- HPV & HSV may participate in oral SCC formation : There has been considerable interest in the role of the human papilloma virus ( HPV) & the herpes simplex (HSV) in the development of oral SCC. Serologic or E/M studies of oral SCC has demonstrated the presence of these viruses in some cases. While it is doubtfull that these organisms acting alone can initiate a cancer , they may act along with other ( alcohol ? Cigarette smoke ? ) to cause malignant transformation “ cocarcinogen”
4- Sunlight exposure is associated in development of lip SCC : Exposure to actinic radiation is clearly associated with development of cancer ( SCC) of the lip. That this cancer affects the lower , not the upper , lip & occurs commonly in those in outdoor occupations , lead to the observation 5- Syphilis : syphilitic leukoplakia developing late in the syphilitic patients . This leukoplakia has high malignant potential . 6- Aging : It has already been mentioned that the incidence of oral SCC becomes more common with increasing age. Clinical picture : old age , sex: male than female , Site : not affect all mouth areas equally . Incidence of SCC by location
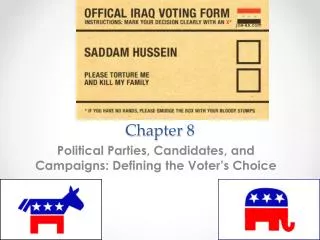
Relative risks of developing oral cancer in consumers (males in a western population) of tobacco and alcohol. The relative risk for a non-smoker and non-alcohol consumer is taken as 1. A smoker consuming 30 cigarettes a day and 20 alcoholic drinks a week is seven times more likely to develop carcinoma.
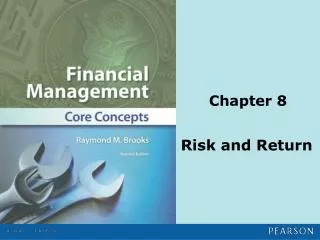
- Commonly affected areas are “ high risk areas” for SCC. - Review of the locations listed in the following table clearly demonstrate that it is the lateral tongue , the ventral tongue , the soft palate , the tonsillar pillars , & the floor of the mouth account for two thirds ( 66%) of the cases of intraoral SCC. -The lips are excluded from this figure because they are not within the mouth ( not intraoral) & because the cure from lip SCC is very high. - On the other hand , the cure rates for intraoral SCC is much lower. - The risks associated with intraoral SCC are so high that “ high risk areas” have been identified . - These high risk areas are 1) the lateral tongue , 2) the ventral tongue , 3) the floor of the mouth , 4) the soft palate , & 5) the tonsillar pillars. - It is essential that dentists & dental hygienists include these areas in intraoral clinical examination.
High risk areas : • Tongue , lateral • Tongue , ventral • Floor of mouth • Soft palate • Tonsillar pillars Intraoral high risk areas for SCC
Characters : - Oral SCC can be recognised by changes in color & texture in the oral mucosa. - Oral SCC arises in the epithelium of the oral mucous membrane. -The changes associated with the development of this malignancy produce changes that can be seen by an observant clinician. - These changes include alterations in colour , texture , & shape of the oral mucous membrane. - The appearance of oral SCC is variable.
-It is dependent on the stage in which it is discovered , how aggressively the neoplasm behaves , & from what part of the mucosa did it arise. - Oral SCC often manifests as a painless , indurated ulcer : -As will be seen later , once a cancer originating in the mucosal epithelium invades the underlying C.T. ( lamina propria) it is designated as being : invasive “ . -In the remainder of that is a centimeter or larger in diameter -The rolled & raised edges of the lesion surround a depressed central region. -The lesion is usually redder than the surrounding mucosa & easily bleeded. -Palpation reveals the lesion to be firm & “ fixed” to the surrounding tissues , a property known as “ induration” .
The margins of ulcer is glazed , the floor is papillomatous with foul odour. - Red , white , or ulcerated lesions : By the time oral SCC becomes a 1cm crated ulcer , invasion has surely occurred & the possibility of metastasis is real. The way to prevent this tragedy , of course , is to discover oral SCC before invasion & metastasis occurs. It turns out , that early changes manifest in a number of different ways. Some lesions are white , some are red & some are speckled red & white. Some are raised above the surface as smooth or papillary or warty projections . And some are small non-indurated ulcers.
Microscopic features : • Microscopically oral SCC usually shows abnormal keratinization. • As it is name was designed to covey , oral “ squamous cell carcinoma “ is malignant neoplasm that arises from covering & lining epithelium ( oral mucous membrane). • The disease probably arises from malignant transformation of “ reserve keratinocytes “ located in the stratum basalis or the stratum spinosum . • Such transformation usually produces a neoplasm that is able to produce some abnormal keratin.
The capability is sign of differentiation ; it is retention means that the neoplasm is a “ moderately – well- differentiated” one. • Epithelial dysplasia = it means abnormal formation of epithelium. Signs of epithelial dysplasia : 1- basilar hyperplasia 2- loss of polarity & disorientation of cells. 3- cell nest formation 4- epithelial pearl & individual cell keratinization 5- abnormal mitosis 6- hyperchromatism of the nuclei
7- alteration of N/C ratio 8- dyskeratosis ( nuclear atypia) 9- poikoilo karynosis ( division of the nucleus without division of the cytoplasm) . 10- large prominent nucleoli. • Keratinization is equated with a “ moderate “ level of differentiation. • Because most oral squamous cell carcinomas are moderately to well differentiated neoplasms & retain some features of keratinization , it is not surprising that most are composed of polyhedral cells displaying “ intercellular bridges” & abnormal keratinization.
Abnormal keratin manifests as whorls of flat keratinized cells called “ keratin pearls” & as orange – staining cells indicating “ individual cell keratinization “ . • The identification of these features are important because they identify the neoplasm as being 1) derived from covering & lining epithelium & being 2) moderately to well – differentiated . • While this pattern is the common theme , from time to time variations occur. • Most of these do not show keratinization & are , therefore , less differentiated forms of the disease. Microscopically , the invasive qualities of SCC can be seen clearly . Despite the level of differentiation , virtually lesions demonstrate invasion of the underlying tissues by groups of epithelial cells , a feature that is
Obvious to the experienced eye. Such invasion may penetrate lymphatic vessels , blood vessels , & nerve sheaths providing metastatic pathway . Treatment : Surgery ; radical surgery may be necessary . - may be treated by radiation with or without surgery , - Chemotherapy : to control dissemination Prognosis : The prognosis depends on it is stage when treated 1- the size tumour T , 2- whether lymph nodes are involved N 3- whether distant has occurred M Staging is accomplished by the TNM systems ,in the following table :
Squamous cell carcinoma of the lip: • The lip is the most common site of oral cancer Defintion : it is a malignant neoplasm arising from stratified squamous epithelium Clinically : age : middle & old age , sex : male more than female 2:1 Site : lower lip > upper lip ( 95% lower lip – 5% upper lip . • Usually begin on the vermilion border to one side of the middle , it starts as a small thickening , induration & ulceration covered with a crust , later ; hard prominent mass , or crater like ulcer • Crater like ulcer : Everted raised edges , Glazed margins , Papillomatous floor , bleeding Foul odour , indurated base. • Rate of growth & histopathology : • Slow or rapid forming a large fungating mass. Most lip carcinomas are grade : & II so : late metastasis to submental or submandibular L.N. , ipsilateral (same side ) or contrlateral
Advanced carcinoma of lip. There is extensive ulceration and necrosis and distortion. Nowadays such extensive lesions are unusual. Squamous carcinoma of lip. There is an indurated, crusted ulcer with keratosis at one margin in the centre of the lower lip.
Squamous carcinoma. Higher power shows strands of malignant epithelium invading the connective tissue. A small squamous carcinoma. At low power the epithelium is seen to invade deeply into the connective tissue and underlying muscle. At this early stage there is no ulceration.
Squamous carcinoma. In this moderately well-differentiated tumour many of the neoplastic epithelial cells are forming keratin pearl Squamous carcinoma. At high power a group of tumour cells shows typical cytologic irregularity. Surrounding and beneath the tumour, muscle fibres are being destroyed. Squamous carcinoma. In this poorly-differentiated carcinoma there is little or no keratin formation and the malignant cells show great pleomorphism with variably-sized nuclei, many of which are hyperchromatic, and frequent mitotic figures.
Squamous carcinoma. Less frequent than perineural invasion is vascular invasion. Here a cluster of poorly-differentiated malignant epithelial cells have eroded the wall of the vessel and entered the circulation. Squamous carcinoma. In this carcinoma malignant epithelium is invading around nerve sheaths. Although this is infrequent, occasionally carcinoma may spread some distance from the main tumour mass along nerve trunks.
Carcinoma of the tongue : Malignant epithelial neoplasm of the tongue • Etiology : Sepsis , spicy food , syphilis , Spirits ( alcohol) , smoking • Clinical picture : Age : middle & old age , sex : male more than female , • Site : lateral border of the anterior part of tongue. • Characters : 1) Exophytic or 2) Ulcer , which infiltrates the deep layers of the tongue , producing fixation & induration , The ulcer has : irregular raised edges , glazed margins , inflammed granulating floor , bleeding , foul odour , indurated base due to infiltration of the surrounding by the tumour & to fibrosis. • The tongue becomes stiff & more painful ( severe pain difficulty in eating , swallowing & talking ) as the growth is fixed & infiltrates the tongue . Involvement of L.Ns is common. • Hidden carcinoma of the tongue : Affect the posterior portion of the tongue & are usually more malignant , metastasis early & offer a poor prognosis.
Signs of hidden Ca of the tongue : 1- Slight deviation of the tongue to the affected side on protrusion ( Deviation ) due to : a- restricted mobility of muscles ( tumour invasion ) b- paralysis of motor nerve 2- Slight defect in speech ( Defective speech ) 3- Slight surface dimpling ( Dimpling ) , or other evidence of mucous membrane retraction. 4- A minute ulcer at the most superficial point ( Defective surfaces ) 5- Bleeding with a disagreeable fetid exudate ( Discharge ) 6- Induration at the base ( Hardness ) Lymphatic drainage : 1- Tip of tongue – submental L.N. 2- Dorsum & sides of tongue – submandibular L.N. 3- Abnormal routes of cancer spread may occur So all L.N of neck must be examined ( L.N become enlarged , hard & fixed ) Metastasis : A- same side ( ipsilateral B- bilateral ( contralateral)
Local spread : Destruction of adjacent parts tongue becomes fixed . Severe pain so swallowing & speech are difficult. Cause of death : 1- Pain & infection cause difficulty in eating. 2- Aspiration of septic material from the mouth ( bronchopneumonia) 3- Haemorrhage 4- Metastasis to vital organs. Histopathology : Poorly differentiated SCC Grade II & grade V
Carcinoma of Maxillary sinus : • It is a very serious disease as it is often advanced before the patient discover it. • Carcinoma of the maxillary sinus may be : • SCC or adenocarcinoma ( originating from the glands in the lining of the sinus ). Clinical features : 1- Swelling of the maxillary alveolar ridge , palate or mucobuccal fold. 2- loosens or elongation of the maxillary molars. 3- Swelling of the face inferior & lateral to the eye. 4- Unilateral nasal bleeding or discharge. 5- Difficulty of wear denture.
VERRUCOUS CARCINOMA : it is a form of SCC of the oral cavity which was defined as an entity. It differs from usual SCC in : 1- slow growth 2- Exophytic growth 3- invade superficially 4- low tendency & late metastasis 5- not aggressive , needs local excision. 6- Always good prognosis. Clinical features : Age : old age 60-70 y , Sex : 75% of lesions develop in males ( tobacco chewing ) , Site : Buccal mucosa , gingiva or alveolar mucosa . Occasionally involves the palate or floor of the mouth. Characters : Papillary or warty lesion covered by a white film. Patient complain of pain & difficulty in mastication . Histopathology : 1- Down growth of proliferating rete ridges. 2- Blunt rete pegs “ push down” but do not invade the underlying tissues. 3- Well differentiated epith. & shows little mitotic activity. 4- Cleft like spaces lined by a thick layer of parkeratin extend from the surface deeply into the lesion. 5- Marked chronic inflammatory cell infiltration in the underlying C.T. Prognosis : much better than usual SCC
Verrucous carcinoma. An extensive lesion covering most of the buccal mucosa and starting to involve the skin at the commissure. Such longstanding lesions are likely to develop invasive squamous carcinoma and may then metastasis. Verrucous carcinoma. The epithelium is thickened and thrown into a series of folds with a spiky parakeratotic surface. Deeply the carcinoma retains a broad pushing front.
2-Transitional cell carcinoma or lymphoepithelioma : - It is very malignant neoplasm. - It runs a rapid clinical course , metastasize rapidly & widely & causes very early death. Clinical pictures : Age : old age , Sex : male more than female. Site : the posterior part of the tongue , the tonsil or the nasopharynx & on the palate. Characters : it may be Very small hidden or slightly elevated or ulcerated . Sore throat , nasal obstruction , defective hearing or ear pain , headach , dysphagia & epistaxis. Metastasis to the regional L.Ns occurs early before medical advice. Histopathology : sheets or cords & nests of : large round or polyhedral cells , with indistinct outlines & large , round nuclei , variable degrees of mitotic activity. The stroma is infiltrated by lymphocytes ( it is very radiosensitive). Treatment : radiation. Prognosis : poor because of early widespread metastasis & early recurrence.
Basal cell carcinoma ( Rodent ulcer ) : It is a locally malignant epithelial neoplasm .It arises from the basal cells. Aetiology : - Ultraviolet rays of sunlight - Commonly affect blond people Clinical features : Age : middle & old age , Sex : more common in males , site : exposed skin surface , scalp & middle third of face . It may reach oral mucosa as it extends from the skin. Characters : Small elevated papule which ulcerate & heals over. Break down again & later on superficial ulcer with smooth rolled border . The lesion invades locally all tissue so it can erode the skull & kill the patient. Histopathology : Nests with indistinct cell membranes or islands of cells with large deeply stained nuclei or sheets with some mitotic figures. - The peripheral cells of each cell nests are well polarized cells that resemble basal cells. - There is no or little tendency to differentiate . - No metastasis - But as the basal cells are pluripotential cells which form hair , sebaceous glands sweat gland. Multiple basal cell carcinoma of the skin are a feature of the jaw cyst , bifid rib , basal cell naevus , syndrome
4- Malignant melanoma • It is the most deadly neoplasm , it arise from junctional nevus Clinical features : Age : after 30 years of age , Sex : equal , Site : skin , eye , vaginal mucosa. • Uncommon oral mucosa ( maxillary alveolar ridge & palate ) , cheek , tongue & floor of mouth. Characters : It appears as enlarging pigmented area often surrounded by an erythematous zone , frequently shows crusting , bleeding or ulceration . • Oral lesion : appears as deeply pigmented area , often ulcerates & bleeds & tend to increase in size.. • Metastasis are common to regional lymph node & to distant sites such as liver & lung. Histopathology : Closely packed cuboidal or fusiform cells arranged in an alveolar pattern , reaching deep in the C.T. , mitotic activity & melanin pigmentation. Treatment : radical surgical resection.
Malignant C.T. neoplasms ( Sarcoma) 1- Fibrosarcoma : it is a malignant fibrous C.T. neoplasm Clinical features : Age : 20-40 years , Sex L equal ,Site : buccal mucosa , palate , lip & jaw Characters : It appears as a fleshy swelling , ulceration , haemorrhage & secondary infection. - it destroys the surrounding structures . - Asymmetric swelling & distortion - Metastasis are not frequent. Histologic features : - Proliferating malignant fibroblasts show anaplasia & mitosis. - Interlacing collagen & reticulin fibers show spiral arrangement . -Thin walled blood vessels. - Giant cells & numerous abnormal mitotic figures in tumours.
Fibrosarcoma of the tongue. There are streams of neoplastic fibroblasts, but the striking feature is the spindle-shaped, darkly staining nuclei and their variation in size and mitoses.
2- Osteogenic sarcoma • It is a primary malignant neoplasm of bone • Unknown etiology but few cases follow irradiation of Paget,s disease of bone. • Age : 10-20 years or old age if associated with Paget,s disease of bone., Sex : male more than female , Site : body of mandible is more than maxilla. • Radiographic : osteoblastic appear as radioopaque osteolytic appear as irregular radiolucent area 3- Chondrosarcoma • It is a malignant neoplasm of cartilage. • Primary chondrosarcoma from the start or secondary from chondroma • Age : 30-60 years , male more than female , site : mandible or maxilla • X ray : radiolucent with radioopaque. 3- Ewing ,s sarcoma : • It is a malignant neoplasm arising from bone marrow endothelium. • Age : 5-25 years , male more than female , site : long bone , skull , clavicle , mandible & maxilla. • Radiograph : onion skin appearance ( due to subperiosteal bone formation )
The most common subtype is osteosarcoma that arises in the metaphysis of long bones; is primary, solitary, intramedullary, and poorly differentiated; and produces a predominantly bony matrix