Download
1 / 13
350 likes | 2.85k Vues
Nikola Blažević Mentor: A. Žmegač Horvat. GRADING AND STAGING OF TUMORS. GRADING. Degree of maturity or differentiation under the microscope Histologic grade – resemblance between tumor and normal cells Nuclear grade – size and shape of nucleus, dividing cells

E N D
Nikola Blažević Mentor: A. Žmegač Horvat GRADING AND STAGING OF TUMORS
GRADING Degree of maturity or differentiation under the microscope Histologic grade – resemblance between tumor and normal cells Nuclear grade – size and shape of nucleus, dividing cells Carcinoma,adrenal gland
How is tumor grade determined? • Biopsy – benign or malignant - pathologist – level of differentiation • http://www.youtube.com/watch?v=Ms4b7eGLtf8&feature=related
TUMORGRADES • Microscopic apperance of cancer cells • 4 degrees of severity • Grade: GX Grade cannot be assessed (Undetermined grade) G1Well-differentiated (Low grade) G2 Moderately differentiated (Intermediate grade) G3 Poorly differentiated (High grade) G4 Undifferentiated (High grade)
GRADING SYSTEMS Different for different types of cancers Gleason – prostate cancer Bloom-Richardson – breast cancer Fuhrman – kidney cancer Gleason system Fuhrman system
GRADING – TREATMENT • For treatment and prognosis • Lower grade better prognosis (outcome of diease) • Higher grade worse prognosis • Important in treatment of prim. brain tumors (astrocytomas) lymphomas breast cancer prostate
STAGING • Extent of the prim. tumor and extent of spread in the body • Important - helps planning treatment - helps estimating prognosis - helps identifying clinical trials
STAGING SYSTEMS • No unique staging system • Common elements : - Location of the primary tumor - Tumor size and number of tumors - Lymph node involvement (spread of cancer into lymph nodes) - Cell type and tumor grade (how closely the cancer cells resemble normal tissue) - Presence or absence of metastasis
TNM - system • Most common (accepted by UICC, AICC) • Based on : T extent of the tumor Nextent of spread to the lymph nodes M presence of metastasis • Number indicates size or extent of the prim. tumor and the extent of spread of metastasis
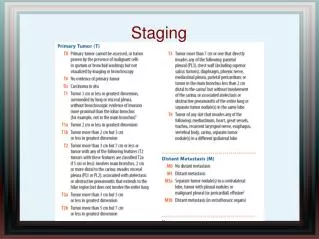
Primary Tumor (T) TX Primary tumor cannot be evaluated T0 No evidence of primary tumor Tis Carcinoma in situ (has not spread) T1, T2, T3, T4 Size and/or extent of the primary tumor Regional Lymph Nodes (N) NXRegional lymph nodes cannot be evaluated N0 No regional lymph node involvement N1, N2, N3 Involvement of regional lymph nodes (number and/or extent of spread) Distant Metastasis (M) MX Distant metastasis cannot be evaluated M0 No distant metastasis M1 Distant metastasis (cancer has spread to distant parts of the body)
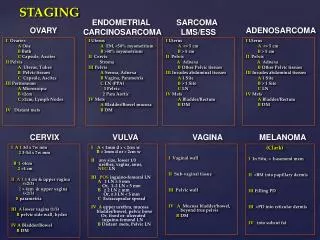
OTHER CLASSIFICATION Ann Arbour lymphomas Duke’s classification colon cancer Breslow scale and Clark’s level melanoma
DETERMINATION OF STAGES Physical exams examination, looking, listening Imaging studies X-ray, US, CT, MRI, PET Laboratory tests blood, urine, AST/ALT, tumor markers (CA19-9,CA19-5….) Pathology reports biopsy, cytology Surgical reports Lung cancer,PET scan
References • http://www.cancer.gov/ • www.wikipedia.com • Oxford handbook of clinical medicine,Murray Longmore