Download
1 / 83
830 likes | 981 Vues
Briefing for the SAMHSA Workgroup on Underage and Problem Drinking. Michael Dennis, Ph.D. Chestnut Health Systems, Normal, IL

E N D
Briefing for the SAMHSA Workgroup on Underage and Problem Drinking Michael Dennis, Ph.D. Chestnut Health Systems, Normal, IL Presentation for the Substance Abuse and Mental Health Services Administration’s (SAMHSA) Workgroup on Underage and Problem Drinking, Rockville, MD. This presentation reports on treatment & research funded by the SAMHSA contract 270-07-0191, as well as several individual CSAT, NIAAA, NIDA and private foundation grants. The opinions are those of the author and do not reflect official positions of the consortium or government. Available on line at www.chestnut.org/LI/Posters or by contacting Michael Dennis at 448 Wylie Drive, Normal, IL 61761, phone: (309) 451-7801, Fax: (309) 451-7763, e-mail: mdennis@Chestnut.Org
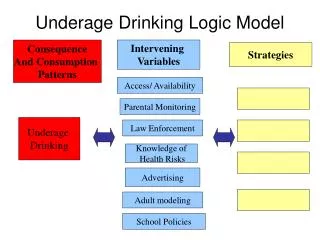
Estimate the size and correlates of underage and problem alcohol use Demonstrate how under age drinking is particularly problematic for youth in the short and long run Show how even a short screener can be used to quickly identify behavioral health problems and impact program planning Describe how the GAIN has been used as a key piece of infrastructure to support the move towards evidenced based practice Illustrate what we have learned by pooling data from CSAT adolescent/young adult grantees and its implications for program planning Goals of this Presentation are to
There 41.4 Million Under Age or Problem Drinkers in the U.S. 17.6 Million under age drinkers (46% of 38.1 Mil) 28.4 Million (12%) Problem Drinkers (4.6m/12% of youth, 23.8m/11% of adult) Source: SAMHSA 2006. National Survey On Drug Use And Health, 2006 [Computer file]
Heavy and Problem Alcohol Use is More Common Among Males 52% 48% Total Population Source: SAMHSA 2006. National Survey On Drug Use And Health, 2006 [Computer file]
Underage, Heavy and Youth Problem Alcohol Use is More Common Among Caucasians 70% 60% Total Population Source: SAMHSA 2006. National Survey On Drug Use And Health, 2006 [Computer file]
Alcohol Use Severity is associated with moreCo-occurring Cannabis Abuse or Dependence Odd Ratio=17.7 Odd Ratio=34.8 5% 1% Total Population Source: SAMHSA 2006. National Survey On Drug Use And Health, 2006 [Computer file]
Alcohol Use Severity is associated with Co-occurring Other Drug Abuse or Dependence Odd Ratio=8.6 Odd Ratio=17.5 3% 1% Total Population Source: SAMHSA 2006. National Survey On Drug Use And Health, 2006 [Computer file]
Alcohol Disorders are associated with Co-occurring Depression Only Alcohol Abuse/Dependence associated with higher Psychiatric Comorbidity Odd Ratio=3.0 Odd Ratio=2.6 19% 11% NOTE: NSDUH does not ask about other disorders or ask about them for those under 18 Total Population Source: SAMHSA 2006. National Survey On Drug Use And Health, 2006 [Computer file]
National Comorbidity Study Replication (NCSR) Shows Comorbidity is Actually More Common (28%/46% Any)= 61% Co-occurring Lifetime Pattern of Disorders Lifetime Number of Disorders (13%/16% SUD)= 81% Co-occurring Source: Dennis, Scott, Funk & Chanforthcoming; National Co morbidity Study Replication
Potential Screening/ Intervention Sites: Age 12 to 20 (38.1 million) Key potential of Workplace (e.g., EAP, Wellness,HRA) and School (e.g., SAP, EI, Prevention) Programs NOTE: Not asked about work if under age 15 in NSDUH Source: SAMHSA 2006. National Survey On Drug Use And Health, 2006 [Computer file]
Potential Screening/ Intervention Sites: Age 21+ (207.9 million) Key potential of Workplace Programs NOTE: Not asked about School if over age 18 in NSDUH Source: SAMHSA 2006. National Survey On Drug Use And Health, 2006 [Computer file]
Severity of Past Year Substance Use/Disorders(2002 U.S. Household Population age 12+= 235,143,246) Dependence 5% Abuse 4% No Alcohol or Regular AOD Drug Use 32% Use 8% Any Infrequent Drug Use 4% Light Alcohol Use Only 47% Source: 2002 NSDUH, Dennis & Scott, 2007
Higher Severity is Associated with Higher Annual Cost to Society Per Person Mean (95% CI) $3,058 This includes people who are in recovery, elderly, or do not use because of health problems Higher Costs $1,613 $1,528 $1,309 $1,078 $948 $4,000 Adults & Adolescents Median (50th percentile) $3,500 $3,000 $2,500 $2,000 $1,500 $1,000 $725 $406 $500 $231 $231 $0 $0 $0 No Alcohol or Light Alcohol Regular AOD Any Dependence Abuse Infrequent Drug Use Use Only Drug Use Use Source: 2002 NSDUH
Severity of Past Year Substance Use/Disorders by Age Over 90% of use and problems start between the ages of 12-20 It takes decades before most recover or die NSDUH Age Groups 100 People with drug dependence die an average of 22.5 years sooner than those without a diagnosis 90 80 70 60 Severity Category 50 No Alcohol or Drug Use Light Alcohol Use Only 40 Any Infrequent Drug Use 30 Regular AOD Use 20 Abuse 10 Dependence 0 (2002 U.S. Household Population age 12+= 235,143,246) 65+ 12-13 14-15 16-17 18-20 21-29 30-34 35-49 50-64 Source: 2002 NSDUH and Dennis & Scott 2007
pain Adolescent Brain Development Occurs from the Inside to Out and from Back to Front Photo courtesy of the NIDA Web site. From A Slide Teaching Packet: The Brain and the Actions of Cocaine, Opiates, and Marijuana.
Crime & Violence by Substance Severity Substance use severity is related to crime and violence Adolescents 12-17 Source: NSDUH 2006
Family, Vocational & MH by Substance Severity ..as well as family, school and mental health problems Adolescents 12-17 Source: NSDUH 2006
Age of First Use Predicts Symptoms of Dependence an Average of 22 years Later 100 Under Age 15 90 Aged 15-17 80 Aged 18 or older 71 70 63 62 60 51 % with 1+ Past Year Symptoms 48 50 45 41 39 37 40 34 30 30 23 20 10 0 Alcohol: Marijuana: Other Drugs: Tobacco: Pop.=151,442,082 Pop.=176,188,916 Pop.=71,704,012 Pop.=38,997,916 OR=1.49* OR=2.74* OR=2.45* OR=2.65* Source: Dennis, Babor, Roebuck & Donaldson (2002) and 1998 NHSDA * p<.05
People Entering Publicly Funded Treatment Generally Use For Decades It takes 27 years before half reach 1 or more years of abstinence or die 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Percent still using Years from first use to 1+ years of abstinence 0 5 10 15 20 25 30 Source: Dennis et al., 2005
The Younger They Start, The Longer They Use 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Percent still using Age of First Use* Years from first use to 1+ years of abstinence under 15 60% longer 15-20 21+ 0 5 10 15 20 25 30 * p<.05 Source: Dennis et al., 2005
The Sooner They Get The Treatment, The Quicker They Get To Abstinence 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Years to first Treatment Admission* Percent still using 20 or more years Years from first use to 1+ years of abstinence 57% quicker 10 to 19 years 0 to 9 years 0 5 10 15 20 25 30 • p<.05 Source: Dennis et al., 2005
Why we need to be expand beyond specialty care into school, work place, and health care.. Few Get Treatment: 1 in 19 adolescents, 1 in 21 young adults, 1 in 12 adults Over 88% of adolescent and young adult treatment and over 50% of adult treatment is publicly funded Much of the private funding is limited to 30 days or less and authorized day by day or week by week Health care reform (including school based health care, prevention care, and equity) may change this Source: OAS, 2009 – 2006, 2007, and 2008 NSDUH
Cost of Substance Abuse Treatment Episode Many SBIRT, School, Workplace and other early intervention programs focus on brief intervention • $750 per night in Detox • $1,115 per night in hospital • $13,000 per week in intensive • care for premature baby • $27,000 per robbery • $67,000 per assault $70,000/year to keep a child in detention $22,000 / year to incarcerate an adult $30,000/ child-year in foster care Source: French et al., 2008; Chandler et al., 2009; Capriccioso, 2004
Investing in Treatment has a Positive Annual Return on Investment (ROI) Substance abuse treatment has been shown to have a ROI of between $1.28 to $7.26 per dollar invested Treatment drug courts have an average ROI of $2.14 to $2.71 per dollar invested This also means that for every dollar treatment is cut, we lose more money than we saved. Source: Bhati et al., (2008); Ettner et al., (2006)
The Movement to Increase Screening Screening, Brief Intervention and Referral to Treatment (SBIRT) has been shown to be effective in identifying people not currently in treatment, initiating treatment/change and improving outcomes (see http://sbirt.samhsa.gov/ ) The US Preventive Services Task Force (USPSTF, 2004; 2007), National Quality Forum (NQF, 2007), and Healthy People 2010 have each recommended SBIRT for tobacco, alcohol and increasingly drugs CSAT, CSAP, OJJDP, BJS NIAAA and NIDA are funding several projects to develop and evaluate models for doing this in primary care, trauma, emergency departments, schools, workplaces, and justice programs Washington State mandated screening in all adolescent and adult substance abuse treatment, mental health, justice, and child welfare programs with the 5 minute Global Appraisal of Individual Needs (GAIN) short screener
Washington State Results with GAIN Short Screener: Adolescent Problems could be easily identified & Comorbidity common Source: Lucenko et al (2009). Report to the Legislature: Co-Occurring Disorders Among DSHS Clients. Olympia, WA: Department of Social and Health Services. Retrieved from http://publications.rda.dshs.wa.gov/1392/
Adolescent Client Validation of Hi Co-occurring from GAIN Short Screener vs Clinical Records by Setting in Washington State Two page measure closely approximated all found in the clinical record after the next two years Source: Lucenko et al (2009). Report to the Legislature: Co-Occurring Disorders Among DSHS Clients. Olympia, WA: Department of Social and Health Services. Retrieved from http://publications.rda.dshs.wa.gov/1392/
Where in the System are the Adolescents with Mental Health, Substance Abuse and Co-occurring? School Assistance Programs (SAP) largest part of BH/MH system SAP+ SA Treatment Over half of system Source: Lucenko et al (2009). Report to the Legislature: Co-Occurring Disorders Among DSHS Clients. Olympia, WA: Department of Social and Health Services. Retrieved from http://publications.rda.dshs.wa.gov/1392/
Washington State Results with GAIN Short Screener: Adults Problems could be easily identified & Comorbidity common Source: Lucenko et al (2009). Report to the Legislature: Co-Occurring Disorders Among DSHS Clients. Olympia, WA: Department of Social and Health Services. Retrieved from http://publications.rda.dshs.wa.gov/1392/
Washington State Validation of Co-occurring: GAIN Short Screener vs Clinical Records Higher rate in clinical record in Mental Health and Children’s Administration. (Important of considering urine tests and other sources of information) Source: Lucenko et al (2009). Report to the Legislature: Co-Occurring Disorders Among DSHS Clients. Olympia, WA: Department of Social and Health Services. Retrieved from http://publications.rda.dshs.wa.gov/1392/
Where in the System are the Adults with Mental Health, Substance Abuse and Co-occurring? Substance Abuse Treatment is over half of treatment system for substance disorders, other mental disorders, and co-occurring Source: Lucenko et al (2009). Report to the Legislature: Co-Occurring Disorders Among DSHS Clients. Olympia, WA: Department of Social and Health Services. Retrieved from http://publications.rda.dshs.wa.gov/1392/
Total Disorder Screener Severity by Level of Care: Adolescents About 30% of OP & SAP are in the high severity range more typical of residential Outpatient & Student Asst. Prog. are Similar (Median 6.0 vs. 6.4) Residential Median (10.5) is higher Well Targeted 95% 1+ 85% 3+ Source: SAPISP 2009 Data and Dennis et al 2006 32
Total Disorder Screener Severity by Level of Care: Adults About 20% of OP are in the high severity range more typical of residential Outpatient Median=4.5 (29% at 10+) Residential Median= 8.5 (59% at 10+) 10% of adult OP missed) Source: SAPISP 2009 Data and Dennis et al 2006 33
GAIN SS Can Also be Used for Monitoring Track Gap Between Prior and current Lifetime Problems to identify “under reporting” Track progress in reducing current (past month) symptoms) 20 12+ Mon.s ago (#1s) 2-12 Mon.s ago (#2s) 16 Past Month (#3s) Lifetime (#1,2,or 3) 11 12 10 10 9 9 8 8 3 4 2 2 0 Intake 3 6 9 12 15 18 21 24 Mon Mon Mon Mon Mon Mon Mon Mon Total Disorder Screener (TDScr) Monitor for Relapse
Use of a short common screener can Provide immediate clinical feedback that is a good approximation of diagnosis and be used to guide placement and treatment planning Can be used repeatedly to track change Support evaluation and planning at program or state level (e.g., needs, case mix, services needed) Provide practice based evidence to guide future clinical decision Be incorporated into health risk/ wellness assessments and/or school surveys
In practice we need a Continuum of Measurement (Common Measures) Screening to Identify Who Needs to be “Assessed” (5-10 min) Focus on brevity, simplicity for administration & scoring Needs to be adequate for triage and referral GAIN Short Screener for SUD, MH & Crime ASSIST, AUDIT, CAGE, CRAFT, DAST, MAST for SUD SCL, HSCL, BSI, CANS for Mental Health LSI, MAYSI, YLS for Crime Quick Assessment for Targeted Referral (20-30 min) Assessment of who needs a feedback, brief intervention or referral for more specialized assessment or treatment Needs to be adequate for brief intervention GAIN Quick ADI, ASI, SASSI, T-ASI, MINI Comprehensive Biopsychosocial (1-2 hours) Used to identify common problems and how they are interrelated Needs to be adequate for diagnosis, treatment planning and placement of common problems GAIN Initial (Clinical Core and Full) CASI, A-CASI, MATE Specialized Assessment (additional time per area) Additional assessment by a specialist (e.g., psychiatrist, MD, nurse, spec ed) may be needed to rule out a diagnosis or develop a treatment plan or individual education plan CIDI, DISC, KSADS, PDI, SCAN More Extensive / Longer/ Expensive Screener Quick Comprehensive Special
Longer assessments identify more areas to address in treatment planning Most substance users have multiple problems 5 min. 20 min 30 min 1-2 hr Source: Reclaiming Futures Portland, OR and Santa Cruz, CA sites (n=192) 37
How does this relate to the move towards Evidence Based Practice (EBP)? EBP means introducing explicit intervention protocols Targeted at specific problems/subgroups and outcomes Having explicit quality assurance procedures to cause adherence at the individual level and implementation at the program level Reliable and valid assessment is needed that can be used to Immediately guide clinical judgments about diagnosis/severity, placement, treatment planning, and the response to treatment at the individual level Drive longer term program evaluation, needs assessment, performance monitoring and program planning Allow evaluation of the same person or program over time Allow comparisons with other people or interventions
Major Predictors of Bigger Effects Found in Multiple Meta Analyses A strong intervention protocol based on prior evidence Quality assurance to ensure protocol adherence and project implementation Proactive case supervision of individual Triage to focus on the highest severity subgroup
Impact of the numbers of these Favorable features on Recidivism in 509 Juvenile Justice Studies in Lipsey Meta Analysis The more features, the lower the recidivism Average Practice Source: Adapted from Lipsey, 1997, 2005
Evidenced Based Treatment (EBT) that Typically do Better than Usual Practice in Reducing Juvenile Recidivism (29% vs. 40%) Aggression Replacement Training Reasoning & Rehabilitation Moral Reconation Therapy Thinking for a Change Interpersonal Social Problem Solving MET/CBT combinations and Other manualized CBT Multisystemic Therapy (MST) Functional Family Therapy (FFT) Multidimensional Family Therapy (MDFT) Adolescent Community Reinforcement Approach (ACRA) Assertive Continuing Care NOTE: There is generally little or no differences in mean effect size between these brand names Source: Adapted from Lipsey et al 2001, Waldron et al, 2001, Dennis et al, 2004
Implementation is Essential (Reduction in Recidivism from .50 Control Group Rate) The best is to have a strong program implemented well The effect of a well implemented weak program is as big as a strong program implemented poorly Thus one should optimally pick the strongest intervention that one can implement well Source: Adapted from Lipsey, 1997, 2005
Percentage Change in Abstinence (6 mo-Intake) by level of Adolescent Community Reinforcement Approach (A-CRA) Quality Assurance Effects associated with intensity of quality assurance and monitoring (OR=13.5) Source: CSAT 2008 SA Dataset subset to 6 Month Follow up (n=1,961) 43
Importance of Targeting on Performance measures 218/224=97% to targeted 553/771=72% unmet need 771/982=79% in need Size of the Problem Extent to which services are not reaching those in most need Extent to which services are currently being targeted Source: 2008 CSAT AAFT Summary Analytic Dataset
Mental Health Problem (at intake) vs. Any MH Treatment by 3 months Source: 2008 CSAT AAFT Summary Analytic Dataset
Why Do We Care About Unmet Need? If we subset to those in need, getting mental health services predicts reduced mental health problems Both psychosocial and medication interventions are associated with reduced problems If we subset to those NOT in need, getting mental health services does NOT predict change in mental health problems Conversely, we also care about services being poorly targeted to those in need.
Residential Treatment need (at intake) vs. 7+ Residential days at 3 months Opportunity to redirect existing funds through better targeting Source: 2008 CSAT AAFT Summary Analytic Dataset
The GAIN is .. A family of instruments ranging from screening, to quick assessment to a full Biopsychosocial and monitoring tools Designed to integrate clinical and research assessment Designed to support clinical decision making at the individual client level Designed to support evaluation and planning at program level Designed to support secondary analyses and comparisons across individuals and programs The GAIN is NOT an electronic health record (EHR), but a component that can interface with and support EHRs.
The GAIN was developed in collaboration with and is used by a wide range of systems in the US.. NH WA VT ME MT MN ND MA OR WI ID SD NY RI MI WY CT PA IA NV NE NJ OH UT IL IN CA DE CO WV MO VA MD KY KS DC NC TN OK NM State or Regional System GAIN-Short Screener GAIN-Quick GAIN-Full No of GAIN Sites AR AZ SC GA AL None (Yet) MS 1 to 14 TX LA 15 to 30 AK 31 to 165 FL HI More in BZ, CA, CN, JP, MX VI PR 3/10 49
Backbone Funded by CSAT to Support Grant Programs: Grantees Using the GAIN from 9/2007 to 6/2010 Individual Grantee(s) State & Individual Grantee(s) NH WA VT ME MT ND MN OR MA ID NY SD WI MI WY RI AAFT CT IA PA ART NE OH NJ ATDC IN NV DC UT CA BIRT IL DE WV VA CO MO JTDC KS MD EARMARK KY EAT NC FDC TN AZ OK JDC NM SC OJJDP AR ORP GA MS AL RCF TX SAC LA SCAN FL AK SCY TCE YORP HI PR VI 50