Retinal Detachments
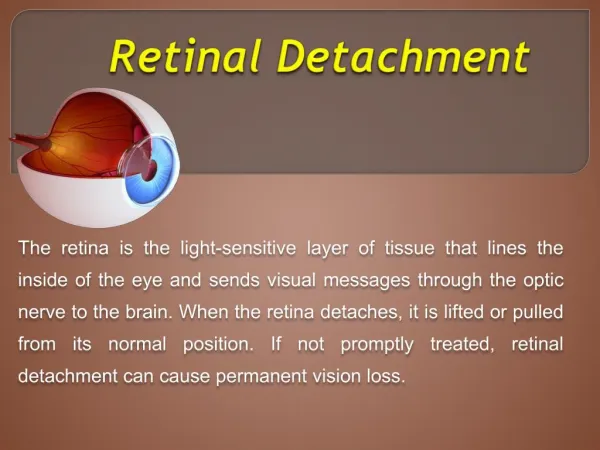
Retinal Detachments. March 18, 2008. Retinal Detachments (RD). Occurs when subretinal fluid accumulates in the potential space between the neurosensory retina and the underlying retinal pigment epithelium (RPE). Classified into rhegmatogenous , tractional , and exudative .

Retinal Detachments
E N D
Presentation Transcript
Retinal Detachments March 18, 2008
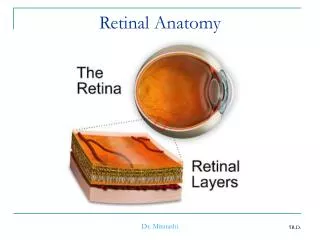
Retinal Detachments (RD) • Occurs when subretinal fluid accumulates in the potential space between the neurosensory retina and the underlying retinal pigment epithelium (RPE). • Classified into rhegmatogenous, tractional, and exudative. • Depends on the mechanism of the subretinal fluid accumulation.
Rhegmatogenous (RRD) • From the Greek rhegma, which means a discontinuity or a break. • Most common type of retinal detachment. • Tear in the retina leads to fluid accumulation with a separation of the neurosensory retina from the underlying RPE.
Pathophysiology of RRD • Fluid from the vitreous cavity can flow through the breaks and detach the retina without there being overt vitreoretinal traction present. • Vitreoretinal traction is responsible for the occurrence of most RRD.
How Likely are RRD’s? • The annual incidence of RRD in the U.S is 12 cases per 100,000 (Haimann et al, 1982 and Wilkes et al, 1982). • Internationally? (Wong et al, 1999) • China: 11.6 cases per 100,000 • India: 3.9 cases per 100,000 • 0.005% to 0.01% of the general population. • Most RRDs occur in persons aged 40-70 years. Why?
History of Concern • Risk factors that predispose to premature PVD. • Myopia (over -5.00 D) • 1% to 3% of high myopes • Prior intraocular surgery • Family history • RRD in the fellow eye • Abnormal vitreoretinal adhesions: • enclosed oral bays, lattice degeneration, and cystic retinal tufts. • Certain Genetic Conditions: • Stickler syndrome, Marfan syndrome, homocystinuria, and Ehlers-Danlos syndrome
Symptoms of RRD • Photopsia • VF defect (“black curtain”, “veil”, “cobwebs”) • Floaters • Ring-shaped floater = Weiss ring • Colored small spots • Loss of Central Vision • The majority of RD’s are asymptomatic.
Typical Exam Findings in RRD’s • Cell and flare in the anterior chamber. • IOP is usually lower in the eye with RRD. • Pigment in the anterior vitreous • “tobacco dusting” or “Shaffer sign” • Retina undulates with eye movements. • Horseshoe or flap tear is often present. • 60% are located in the upper temporal quadrant. • 15% are located in the upper nasal quadrant
Other Examination Pearls • Look for obscuration of underlying choroid • A wide view is helpful (60º view) • Have the patient move their eyes. • Scleral indentation or depression.
Exudative RD’s • Normally - water flows from the vitreous cavity to the choroid. • Relative hyperosmolarity of the choroid with respect to the vitreous. • RPE actively pumps ions and water from the vitreous into the choroid. • A breakdown of this fluid flow leads to Exudative RD.
Appearance of ERD’s • Appears more solid. • No folds like that seen in RRD’s. • Anterior segment may show signs of inflammation. • Depends on the underlying cause. • Hard exudates seen in chronic cases.
Causes of ERD’s • Idiopathic • Coats disease, Central serous chorioretinopathy • Inflammatory • Syphilis, Scleritis, vasculitic entities (rheumatoid arthritis, Wegener granulomatosis) or uveitic conditions. • Congenital • Colobomas of the optic nerve • Neoplastic • Choroidal melanoma • Iatrogenic • Excessive panphotocoagulation, Scleral buckling
Other Useful Tests • Ultrasound: • choroidal thickness, presence or absence of choroidal masses • Fluorescein angiography: • central serous chorioretinopathy (“smoke stacking”)
Tractional RD’s • Second most common type of retinal detachment after a rhegmatogenous retinal detachment (RRD). • Secondary to proliferative vitreoretinopathy (PVR) and penetrating trauma, contractile vitreoretinal, epiretinal, intraretinal or subretinal membranes pull the neurosensory retina away from the RPE.
Causes of TRD’s • Proliferative diabetic retinopathy (PDR) • Sickling hemoglobinopathies • Retinal venous obstructions • Retinopathy of prematurity (ROP) • Conditions characterized by progressive retinal ischemia.