Central Line insertion
What’s New For the Millennium?. Central Line insertion. Dr. David Easton MD FRCPC . University of Manitoba, Canada Section of Critical Care and Emergency Medicine Winnipeg Regional Health Authority Critical Care Quality Committee. Introduction.

Central Line insertion
E N D
Presentation Transcript
What’s New For the Millennium? Central Line insertion
Dr. David Easton MD FRCPC University of Manitoba, Canada Section of Critical Care and Emergency Medicine Winnipeg Regional Health Authority Critical Care Quality Committee
Introduction • Patient Safety in ICU is one of the “Hot” and area of focus for the New Millennium • Multiple interventions in multiple areas are being proposed and adopted to help improve care/outcomes and prevent complications • The Institute for Hospital Improvement (IHI) is a driving force in North America
Introduction • Central Line Insertion is a area of focus and there are two main areas that can reduce complications and improve patient outcomes • Preventing Central Line Infections using a “Central Line Quality Bundle” • Ultrasound guided Central Line Insertion
Goals & Objectives • Review components of Central Line Insertion Bundle • Review indications and evidence for ultrasound assisted vascular access • Review basic sonographic technique of ultrasound assisted line insertion
Central Line Infections (CLI) Why Should I care?
Central Line Infections (CLI): • CLI’s – Common! • 50% patients in ICU have Central Venous Catheter (CVC) • Infection rate is 2-5 /1000 catheter days • That equals up to 80,000 infections/yr U.S.A. • CLI’s – Costly! • 2.3 billion dollars/yr U.S.A. • CLI’s – Lethal! • 28,000 patients/yr die from infection
CLI Risk Factors • Site of insertion: Subclavian vein less risky than internal jugular or femoral vein • Multiple ports/hubs: More manipulation and contamination • Parenteral feeding: TPN and/or lipids • Infection elsewhere: Remote source of sepsis already established Mermel LA, Am J Med. Sep 16 1991;91(3B):197S-205S McCarthy MC, J Parenter Enteral Nutr 1987; 11:259.
Central Line Infections • Important Quality Health Care Topic! • In 2002 CDC made recommendations for insertion to help prevent infection • O’Grady, MMWR 2002 • Central Line Insertion Bundle Developed • What is a bundle? • A group of evidence based concepts/guidelines that together improve the outcome of interest
The Central Line Bundle • 5 Simple Steps that have been shown to decrease rates of CLI dramatically • Hand Hygiene –Wash your hands! • Full Barrier Precautions – Fully gown/drape • Clean Skin with Chlorhexidine • Avoid Femoral Line Site – Subclavian best • Remove Unnecessary Lines ASAP
What are Maximal Barrier Precautions? • For the Provider: • Hand hygiene • Non-sterile cap and mask • Sterile gown and gloves • For the Patient: • Cover patient’s head and body with a large sterile drape • “Head to Toe” coverage
But, Does All This Work? ICUs that have implemented the central-line bundle have nearly eliminated CLI’s ! Berenholtz et al. Critical Care Medicine. 2004; 32:2014-2020.
Background • First report of ultrasound to assist in vascular access was by Legler in 1984 in anesthesia literature • found was similar to landmark technique
Background • Experience and research has grown overtime • In 2007 - Over 200 papers on subject • Currently there are numerous guidelines and statements from various organizations across the World
What Is The Basic Evidence? • Adrienne and Cook et al “US guidance for placement of CVC - Meta-analysis” • Used 8 of 208 studies • Found evidence of: • decreased attempt rate • decreased complication rate • decreased failure rate • NNT = 7 to prevent one complication • NNT = 5 to prevent more than 1 attempt Crit Care Med, Dec 1996
…Evidence • Peripheral Access? • “Ultrasound guided brachial and basilic vein cannulation in ED pts” • 100 pts with 2 previous failed attempts • 91% success on first attempt within 90 secs Keys et al, Ann EM, Dec 99
National Guidelines • American - AHRQ report of patient safety 1999: • Evidence based review of new health care technologies • Reviewed 79 safety practices in detail • #8 on list was US guided CL insertion Agency for Health Research & Quality
National Guidelines • UK - National Institute for Clinical Excellence (NICE) NHS - 2002 Guideline statement • 20 randomized clinical trials • Failed catheter placement risk was reduced by 86% • Associated complications reduced by 57% • First attempt success increase by 41% • “Ultrasound is recommended as preferred method of inserting central venous catheters into IJ vein”
Summary • Why should you use Ultrasound? • Increased success rates • Avoids complications • Reduces time to cannulation • Reduces number of attempts • Ultimately safer • And its FUN!
Technique for Use • Some cautions: • We will briefly review technique • One must have dedicated time to practice and have hands on training • Complications are only reduced if operator is skilled in techniques!
Orientation • Probe Position • Transverse and longitudinal • Transverse most useful – lateral orientation • Longitudinal – depth and slope • Can see back wall perforation Trans Long
Transducer contacts skin Deeper or away from the skin
Longitudinal Axis Groove towards Needle Orientation marker Skin surface Blood vessel Head Feet
Image Interpretation • Low density objects like blood vessels appear black • High density objects like bone appear white • Medium density objects like muscle appear gray
Image Interpretation • Identifying Artery vs Vein on Ultrasound • Key to success! • VEINS ARE: • Compressible • Thin and irregular walled compared to artery • Not pulsatile (IJ may have triphasic waves) • Varies with respiration
IJ vein Carotid art
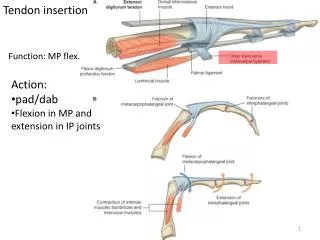
Subclavian Anatomy • Deep to clavicle • Can be hard to image due to depth and patient habitus • Consider lateral approach using axillary vein
Subclavian Anatomy • The lateral approach: • A more lateral and inferior approach • Cannulate the Axillary vein • Can see more easily with ultrasound • Avoids lung and great vessels
Ax V & A Lung!
Technique • Two Main Approaches: • Static • Dynamic or Real Time
Technique • Static Approach • Position patient • Use u/s to locate vessels and mark skin • Avoids complicated hand position/sterile issues
Technique • Dynamic Approach • Real time cannulation under ultrasound visualization • Sterile sleeve placed on probe • Often needs 2 people • Better technique
Technique • In General: • Position patient and get comfortable • Place probe on neck in transverse • Sweep area and ID structures • Place vessel in middle of SCREEN - Vessel should now be in middle of PROBE