Chronic Liver Disease
Chronic Liver Disease. Chronic Liver Disease. Outline: Definition Epidemiology Clinical Presentation History/PE Labs Radiographs Management of complications Ascites (including HRS, SBP) HE Variceal hemorrhage HCC. CLD- Pathophysiology.


Chronic Liver Disease
E N D
Presentation Transcript
Chronic Liver Disease Outline: Definition Epidemiology Clinical Presentation • History/PE • Labs • Radiographs Management of complications • Ascites (including HRS, SBP) • HE • Variceal hemorrhage • HCC
CLD- Pathophysiology When the liver is injured, inflammatory cells infiltrate into the liver leading to the damage of hepatocytes, which is termed ‘‘hepatitis.’’ When the injury, regardless of its cause, is prolonged, numerous mechanisms are initiated to promote healing. Injured areas become surrounded by scar tissue formed by excessive deposition of extracellular matrix as a result of activated fibrogenic mechanisms. These processes may lead to fibrosis, which after a period of time leads to irreversible distortion of the hepatic architecture, termed ‘‘cirrhosis.’’ Fibrosis develops in almost all patients who have chronic liver injury, albeit at variable rates depending on numerous patient factors and the underlying liver disease. Over time, progressive fibrosis ultimately may cause cirrhosis.
CLD/Cirrhosis - Definition The word cirrhosis, derived from the Greek term ‘‘kirrhos,’’ refers to a diffuse process in the liver characterized by the development of extensive fibrosis and replacement of the normal hepatic architecture by structurally abnormal nodules of fibrotic tissue. This structural change in the hepatic architecture eventually leads to functional changes that are characterized collectively as the syndrome of chronic liver failure (CLF). Presence of these changes for more than 6 months distinguishes CLF from acute liver failure
Chronic Liver Disease Cirrhosis Decompensation HCC Malnutrition Pulmonary (HE, ascites, VH) Compl. (HPS, PPH)
Burden of Liver Disease in U.S. Prevalence of 5.5 million cases of CLD/cirrhosis in U.S. Rate of 2030 cases per 100,000 persons Over 60% of cases are male Over 80% are between the ages of 25 and 64 years Little variation in prevalence among different racial or ethnic groups
Leading Causes of Death in U.S. • Chronic liver disease and cirrhosis ranks 12th • Age 35-44 years, ranks 7th • Age 45-54 years, ranks 4th • Age 55-64 years, ranks 7th • Among Hispanics, ranks 7th • Among Native Americans, ranks 6th • Among Native Americans ages 35-44 years, cirrhosis is the 2nd leading cause of death
Economic Impact of Chronic Liver Disease in the U.S. • $1.5 billion in direct annual costs • Inpatient stays • $134 million in physician fees • $1.1 billion in facility fees • Office visits $64.8 million • Medications used to treat CLD/cirrhosis $16.9 million • $234 million in indirect annual costs
Etiology Chronic Liver Disease Common: Nonalcoholic Fatty Liver Disease (NAFLD/NASH) Alcoholic liver disease Chronic hepatitis C (CHC) Chronic hepatitis B (CHB)
Etiology Chronic Liver Disease Less Common: • Autoimmune hepatitis • Primary biliary cirrhosis (PBC) • Primary sclerosing cholangitis (PSC) • Drug-induced hepatitis • Genetic • Hereditary hemochromatosis • α 1 antitrypsin deficiency • Tyrosinemia • Urea cycle disorders • Glycogen storage diseases
Etiology Chronic Liver Disease Other/Miscellaneous: Secondary biliary cirrhosis Sarcoidosis Polycystic liver disease Schistosomiasis Idiopathic portal fibrosis (hepatoportal sclerosis) Cardiac cirrhosis Veno-occlusive disease (sinusoidal obstruction syndrome) Budd-Chiari Syndrome
Etiology of Newly Diagnosed CLD in U.S. GI Practices (Am J Gastro 2008)
Deaths due to CLD • HCC: • 16,780 deaths in U.S. in 2007 • Third leading cause of death from cancer worldwide Hepatology 2006
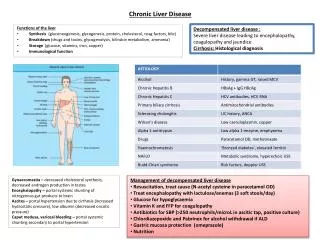
Clinical Presentation History: • Usually asymptomatic • Primary focus is on risk factors of CLD • Alcohol history • Jaundiced illnesses • IVDU, blood transfusions pre-1991, tattoos, incarcerations • Metabolic syndrome • IBD • Other autoimmune disease • Family history • Medications including OTCs and CAM
Clinical Presentation Physical Exam: • “stigmata of chronic liver disease” • Hepatomegaly/splenomegaly • Palmar erythema • Vascular spiders • Dupuytren’s contracture • Terry’s nails/leukonychia • Gynecomastia • Asterixis • Ascites • Fetor hepaticus
Clinical Presentation Labs: • “liver function” is a misnomer • LFT at NMCSD includes: t.bili, d.bili, alt, ast, alk phos, ldh, albumin, t.protein • Markers of hepatic synthetic function include: prothrombin time, albumin, bilirubin • Important considerations: • Duration of abnormality • Degree of elevation (mild ALT<250, severe ALT>1000) • Pattern: hepatocellular, cholestatic, mixed
Clinical Presentation Labs: • Hepatocellular pattern: • Elevation in ALT and AST • ALT(xULN)/AP(xULN) ratio = 5 or greater • Cholestatic pattern: • Elevation in alkaline phosphate (+/-t.bili) • Other cholestatic enzymes include GGT and 5’NT • ALT/AP ratio = 2 or less • Mixed pattern: • Elevation in transaminases and alkaline phosphatase • ALT/AP ratio = >2 and < 5
Clinical Presentation Hepatocellular • Viral hepatitis • AIH • NAFLD • ALD • DILI • Hereditary (HH, A1AT, Wilson’s, celiac sprue) • Ischemic hepatopathy • Congestive hepatopathy • Budd-Chiari • SOS/VOD • Celiac Cholestatic • Extrahepatic biliary obstruction • PSC • PBC • DILI • Sepsis • Post-operative, benign • Infiltrative (sarcoid, lymphoma, tb, amyloid)
Clinical Presentation Labs (specific serologies): CHC: anti-HCV, HCV RNA CHB: HBsAg, HBV DNA PBC: Antimitochondrial Ab (AMA) AIH: ANA, anti smooth muscle Ab (ASMA), IgG HH: ferritin, iron saturation, HFE mutation Wilson’s: ceruloplasmin, 24h urine copper A1AT deficiency: A1AT level/phenotype Celiac: anti-ttg
Clinical Presentation Labs (nonspecific): • AST:ALT of > 1 (even in setting of normal values) • APRI (AST to platelet ratio index) • (AST/AST ULN)/Plt count x 100 • APRI threshold of 0.5 has sens. of 81% and spec of 50% of predicting advanced fibrosis in patients with CHC • Low albumin • Prolonged PT/INR • Thrombocytopenia/Leukopenia • Macrocytosis
Clinical Presentation Radiographic Studies: • Ultrasound • First study of choice (inexpensive, easy) • CT • Liver protocol (triple phase constrast study) • MR • With gadolinium enhancement • Can combine with MRCP
Clinical Presentation Radiographic Studies (findings): • Hepatomegaly • Increased echogenicity (hallmark of steatosis) • Hypodense compared to spleen (steatosis on CT) • Nodular contour liver edge • Left/Caudate lobe hypertrophy • Caudate/Right lobe ratio > 0.65 is 90% specific for cirrhosis • Splenomegaly • Spleen length > 12cm consistent with Portal HTN
Clinical Presenation Radiographic Studies (findings): • Portal vein diameter • >12 mm consistent with Portal HTN • Ascites • Can detect as little as 50ml • Venous collaterallization • Recanalized umbilical vein, varices • Portal vein thrombosis • Bowel wall thickening • 64% of cirrhotics vs. 7% controls • HCC • Early aterial enhancing nodules with venous phase washout
Chronic Liver Disease Cirrhosis Decompensation HCC Malnutrition Pulmonary (HE, ascites, VH) Compl. (HPS, PPH)
Cirrhosis: management(general principles) • Addressing underlying disease • Assessing severity • Prognosis • Natural history • Screening/Surveillance of HCC and varices • Treat decompensation (ascites, HE, etc.) • Preventive
Assessing Severity of Underlying Liver Disease • An accurate assessment of extent and severity of liver disease is required for every cirrhotic • Two commonly used clinical scoring schemes have both been found to correlate with liver-related mortality • Child-Turcotte-Pugh (CTP) • Model for End-Stage Liver Disease (MELD)
Assessing Severity of Underlying Liver Disease CTP: • 1964, Child & Turcotte introduced a scoring system to predict mortality in patients undergoing portocaval shunt surgery • 5 significant factors that affected mortality • Ascites • Albumin • Bilirubin • Encephalopathy • Nutritional status • 1972, Pugh substituted the most subjective factor (nutritional status) with prothrombin time
Modified Child-Pugh Score Points* *Class A = 5-6 points, B = 7-9 points, C = 10-15 points **For cholestatic disorders (eg, PBC) assign 1 point for bilirubin < 4mg/dl, 2 points for 4-10mg/dl, and 3 points for >10mg/dl
Assessing Severity of Underlying Liver Disease MELD: • Originally devised as a prognostic measure of short term mortality in patients undergoing transjugular intrahepatic portosystemic shunt¹ • Patients are assigned a score of 6-40 • The score incorporates 3 biochemical variables • Total bilirubin • Serum creatinine • INR (¹Malinchoc, Hepatology 2000)