Download
1 / 19
190 likes | 286 Vues
Navigate the complexities post-diagnosis from medical appointments to family support. Explore strategies for coping, seeking treatment, and finding comfort through open communication and palliative care. Discover ways to address challenges and uncertainties about end-of-life discussions.

E N D
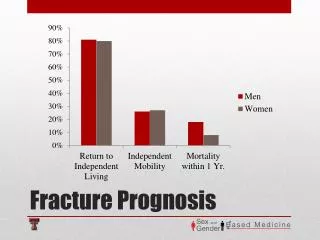
ADJUSTING TO YOUR PROGNOSIS • Jane Turner • Discipline of Psychiatry • School of Medicine
FACING AN • UNCERTAIN FUTURE
IN THE BLINK OF AN EYE • “We were excited. We were sitting with friends on the verandah making plans for Tony’s birthday, just sitting around and relaxing. • Jack said that he would pop down to the frig to get some cold drinks. When he stood up he said he didn’t feel well. Then he collapsed. • The trip to hospital felt like a dream. People everywhere. Tests. Lots of doctors. Going to have a CT scan. Then the news – just like that. • And life was never the same again.” • Helen, aged 42 years
THE CHALLENGE OF THE DIAGNOSIS • Never anticipated • “Like being hit by a cosmic 4X2” • Complexity of medical appointments - who are all these people? • Waiting for information - getting information you can understand • Waiting for results • Telling family and friends • Making treatment decisions • Coping with treatment
WHAT MIGHT HELP? • In general, an active problem-solving approach helps • Brain Tumour Alliance Australia: • http://www.btaa.org.au/ • 1800 857 221 • Fatigue often leads to a cycle of rest, deconditioning and lower energy • Expressing feelings is generally helpful: • No evidence that “being positive” will affect the outcome • There are “tears to be shed” • Open communication is important for families • The truth hurts but secrets hurt more
Support from others is helpful, but others may not always know how to be supportive: • Feel free to ignore people who urge you to “be positive” • Feel free to ignore people who tell you “I knew someone who had that cancer and he/she…..” • Feel bold to ask for what is helpful • Think about some “stock answers” for difficult situations e.g. the persistent/intrusive questioner
Depression and anxiety are common • Effective treatments are available • Often due to a combination of factors: • The diagnosis • Effect of surgery • Effect of radiotherapy • Effect of chemotherapy • Steroids • Past history • Other life stresses • Financial strain
Challenges posed by physical demands e.g. inability to drive • Frustration of dependence on others • Lack of awareness of others “but he looks OK” • Changes in memory especially challenging: • Need to re-think questions/requests • Only when you are face-to-face! • Reduce burden of decision-making/choices • Remember interpolation of words • Go with it rather than struggle for the word • Singing
Coping with personality changes: • More challenging if the person is not aware • If aware can negotiate a signal for “listen to me” • Distraction • Seeing warning signs • Reducing factors which increase difficulty such as fatigue, pain, hunger • Having some time to “recharge the batteries”
SOME SPECIFIC ISSUES • Temporo-parietal problems: • Spatial issues • Dressing • Calculation • Knowing right from left • Executive function: • Planning and decision-making • Self-monitoring and self-correction • Initiation and completion of activities • Responding to novel situations • Reasoning and problem-solving • Ability to inhibit impulses based on current need
PALLIATIVE CARE =“TERMINAL CARE” • Palliative care is a specialty area of health care • It does not mean “terminal care” • Focus is on the unique needs of the individual and their family • Aim is to improve quality of life • Attention to practical, supportive, psychosocial and spiritual needs • Common for people to have periods of needing palliative care interspersed with intervals where palliative care is not required • People receiving palliative care can still have ongoing treatment such as chemotherapy or radiotherapy • Early referral means that there is a “safety net”
“They arrived just after 4 pm – I remember it was a Friday afternoon, and I had thought they would be in a rush to get away for the weekend. But it was like they had all the time in the world. As though we were the only ones who mattered. And for the first time in weeks I could just feel myself breathe, and be calm. I knew that they would look after us.” • Angela, aged 37 years
SOCIETY AND DEATH • We are not good at talking about this! • We use euphemisms to avoid the emotions • Society sanitises things which inhibits us from being to talk about how things really are: • The cancer “fight” • “Brave to the end” • People “pass away” with loved ones at their side • Then people have “closure” – whatever that is!
To ask or not to ask? • There is no certainty about prognosis • Averages are just that - some people will do exceptionally well • Most people say that knowing even bad news allows them to prepare and make decisions • Important to talk with family about what matters: • Reduces burden of family making decisions and worrying “if it is the right thing” • Reduces the chance of regrets
People have a number of very important hopes when they are facing death: • They hope not to die alone • They hope not to suffer • They hope not of have pain • They hope to be able to live whatever time they have left with meaning and joy and purpose • They hope not to be a burden to others • They hope to be remembered • Breitbart & Heller • Journal of Palliative Medicine 2003;979-988
Some final thoughts: • The script is lousy but you are in the director’s chair • There is no right or wrong way - there is just what works for you and your family • If you can’t be selfish now when can you? • Don’t be afraid to seek help to share the burden