SCA-NSTE
490 likes | 694 Vues
SCA-NSTE. considerazioni conclusive: la sintesi per una proposta razionale. Dott. Marco Tubaro Unità Coronarica – Dipartimento Cardiovascolare Ospedale San Filippo Neri – Roma. MT. S CA-NSTE in Lombardia, Friuli Venezia Giulia ed Emilia Romagna.

SCA-NSTE
E N D
Presentation Transcript
SCA-NSTE considerazioni conclusive: la sintesi per una proposta razionale Dott. Marco Tubaro Unità Coronarica – Dipartimento Cardiovascolare Ospedale San Filippo Neri – Roma MT
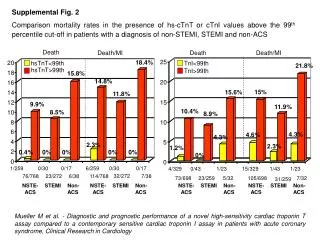
SCA-NSTE in Lombardia, Friuli Venezia Giulia ed Emilia Romagna proporzione SCA-NSTE/STEMI STEMI mortalità SCA-NSTE MT FIC SCA-NSTE, GIC 2009
reparto di ricovero e mortalità MT FIC SCA-NSTE, GIC 2009
linee guida ESC: stratificazione del rischio nelle SCA NSTE elevated troponin levels dynamic ST-T changes (symptomatic or silent) diabetes renal dysfunction (GFR < 60 mL/min/1.73 m2) EF < 40% early post-infarction angina prior MI PCI within 6 months prior CABG GRACE score: intermediate - high mt
routine vs selective invasive strategies in NSTEACS - a metanalysis of 7 trials - OR (95% CI) MT Mehta SR JAMA 2005
ICTUS: intended invasive strategy vs actual revascularization MT Hirsch A. Eur Heart J 2008
MASCARA: early invasive strategy in NSTEACS high risk low-intermediate risk MT Ferreira-Gonzales I. Am Heart J 2008;156:946.
TIMACS: early vs delayed invasive intervention in ACS MT Mehta SR. NEJM 2009;360:2165.
strategies in high risk NSTEACS - PRESTO ACS Registry - MT Tubaro M, ESC Congress 2008
TACTICS: elderly patients NNT 250 21 9 MT Bach RG. Ann Intern Med 2004;141:186
considerazioni per il trattamento degli anziani con SCA NSTE MT Alexander KP, Circulation 2007
gender and therapeutic strategies in NSTEACS - a metanalysis of 8 studies - MT O'Donoghue M. JAMA 2008;300:71.
SWEDEHEART: funzione renale e mortalità MT Szummer K. Circulation 2009;120:851
SWEDEHEART: funzione renale e procedure di rivascolarizzazione MT Szummer K. Circulation 2009;120:851
variabili di rischio e strategia invasiva BLITZ 2 FIC – SCA NTE utilizzo della rete età > 75 anni Killip > 1 diabete troponina PAS < 100 mmHg CORO immediata - angina refrattaria o ricorrente - instabilità emodinamica - instabilità elettrica (TVS, FV) CORO < 24 ore - GRACE > 140 - > 3 variabili di rischio > 3 variabili 17% eventi a 30 gg MT FIC SCA-NSTE, GIC 2009
GRACE: use of interventions according to risk MT Fox KAA. Heart 2007;93:177.
CRUSADE: early (< 48 h) transfer pattern in NSTEACS low risk moderate risk high risk MT Roe MT. Am Heart J 2008;156:185
hs cTnI nella diagnosi precoce dell'IMA MT Keller T. NEJM 09
cTnT nell'insufficienza cardiaca cronica stabile Val-HeFT 100 80 60 40 20 0 92.0 elevated cTnT (% pts) 10.4 cTNThs cTnT DL < 0.01 DL < 0.001 ng/mL ng/mL MT Latini R Circulation 2007
clopidogrel nelle SCA CURE PCI-CURE N Engl J Med 2001 MT Mehta SR. Lancet 2001
CREDO: clopidogrel loading dose timing MT Steinhubl SR. JACC 2006
variability in platelet responsiveness to clopidogrel MT Serebruany, JACC 2005
Cyt P 450 polymorphism & response to clopidogrel MT Mega JL, NEJM '09
attività piastrinica residua con clopidogrel e outcome nelle SCA con stent MT Marcucci R. Circulation 2009
resistenza ai farmaci antipiastrinici (attività piastrinica residua) MT Kuliczkowski W. EHJ 2009
PRINCIPLE TIMI 44: prasugrel vs high dose clopidogrel MT Wiviott SD, Circulation 2007
TRITON TIMI 38: risultati di efficacia e sicurezza MT Wiviott SD. N Engl J Med 2007;357:2001
TRITON TIMI 38: emorragie MT Wiviott SD. N Engl J Med 2007;357:2001
TRITON-TIMI 38 Efficacy and Safety: Post-hoc Analysis for Age, Body Weight, and Prior Stroke/TIA History Adapted from Wiviott et al. NEJM 2007;357:2001-2015
PLATO: ticagrelor vs clopidogrel in ACS primary end-point major bleedings MT Wallentin L, NEJM 2009
PLATO: non-CABG and CABG-related major bleeding 9 Ticagrelor Clopidogrel NS 7.9 8 7.4 7 NS 5.8 6 5.3 p=0.026 5 K-M estimated rate (% per year) 4.5 3.8 4 p=0.025 2.8 3 2.2 2 1 0 Non-CABGPLATO majorbleeding Non-CABGTIMI major bleeding CABGPLATO major bleeding CABG TIMI major bleeding MT Wallentin L, NEJM 2009
Troponin level and benefit with abciximab abciximabvsplacebo death/MI/UTVR 20 troponin +ve: RR=0.71 [0.54-0.95] 15 % 10 troponin -ve: RR=0.99 [0.56-1.76] 5 0 0 5 10 15 20 25 30 days after randomization MT Kastrati A et al. JAMA 2006;295:1531-38
tirofiban nelle sindromi coronariche acute e nella PCI - metanalisi - morte / IMA 0.69 (0.55-0.89) tirofiban upstream vs. P 0.56 (0.37-0.84) tirofiban HD bolus downstream vs. P 0.87 (0.56-1.35) tirofiban HD bolus vs. abciximab 0.4 0.6 0.8 1.0 1.2 1.4 vantaggio tirofiban vantaggio controllo MT Valgimigli M, Eur Heart J 2009
OASIS 5 – emorragie maggiori a 9 giorni Enoxaparin 0.04 HR 0.52 95% CI 0.44-0.61 P<<0.00001 0.03 Cumulative Hazard 0.02 Fondaparinux 0.01 0.0 0 1 2 3 4 5 6 7 8 9 N Engl J Med 2006; 354, 1464-76 MT Days
OASIS 5 – outcome (efficacia) a 6 mesi P=0.055 P=0.036 P=0.037 P=0.33 P=0.029 P=0.005 0.8 1 1.2 MT
ACUITY: età, rischio emorragico e bivalirudin MT Lopez RD, AJC 2009
PRESTO ACS: vascular substudy MT Sciahbasi A. Am J Cardiol 2009
confronto delle linee guida "NSTEACS" di ESC e di ACC/AHA * plus UFH in case of PCI MT
terapia antitrombinica nel post-infarto 728 pazienti, 50-75 aa, QWMI 6-18 mesi eparina calcica 12.500 UI x 2/die follow-up 708+265 gg re-IMA morte morte CV 0 10 20 30 40 50 60 70 riduzione % - 33 % - 48 % - 63 % MT Neri Serneri, Lancet 1987
formazione di trombina dopo SCA MT Merlini PA, Circulation 1994
ATLAS TIMI 46: rivaroxaban nelle SCA MT Mega JL. Lancet 2009
Conclusioni i pazienti con NSTE SCA sono sempre più numerosi e la loro prognosi non è migliorata con gli anni la strategia precocemente invasiva è da riservare prevalentemente ai pazienti ad alto rischio (utilizzando la rete dello STEMI, quando necessario) ai pazienti anziani devono essere riservate cure ugualmente intensive, anche se attente al loro rischio globale nei pazienti ad alto rischio ischemico: prasugrel (e ticagrelor) nei pazienti ad alto rischio emorragico: clopidogrel, fondaparinux, bivalirudin l'approccio radiale è sempre preferibile la terapia anticoagulante a lungo termine potrebbe costituire un progresso ulteriore mt